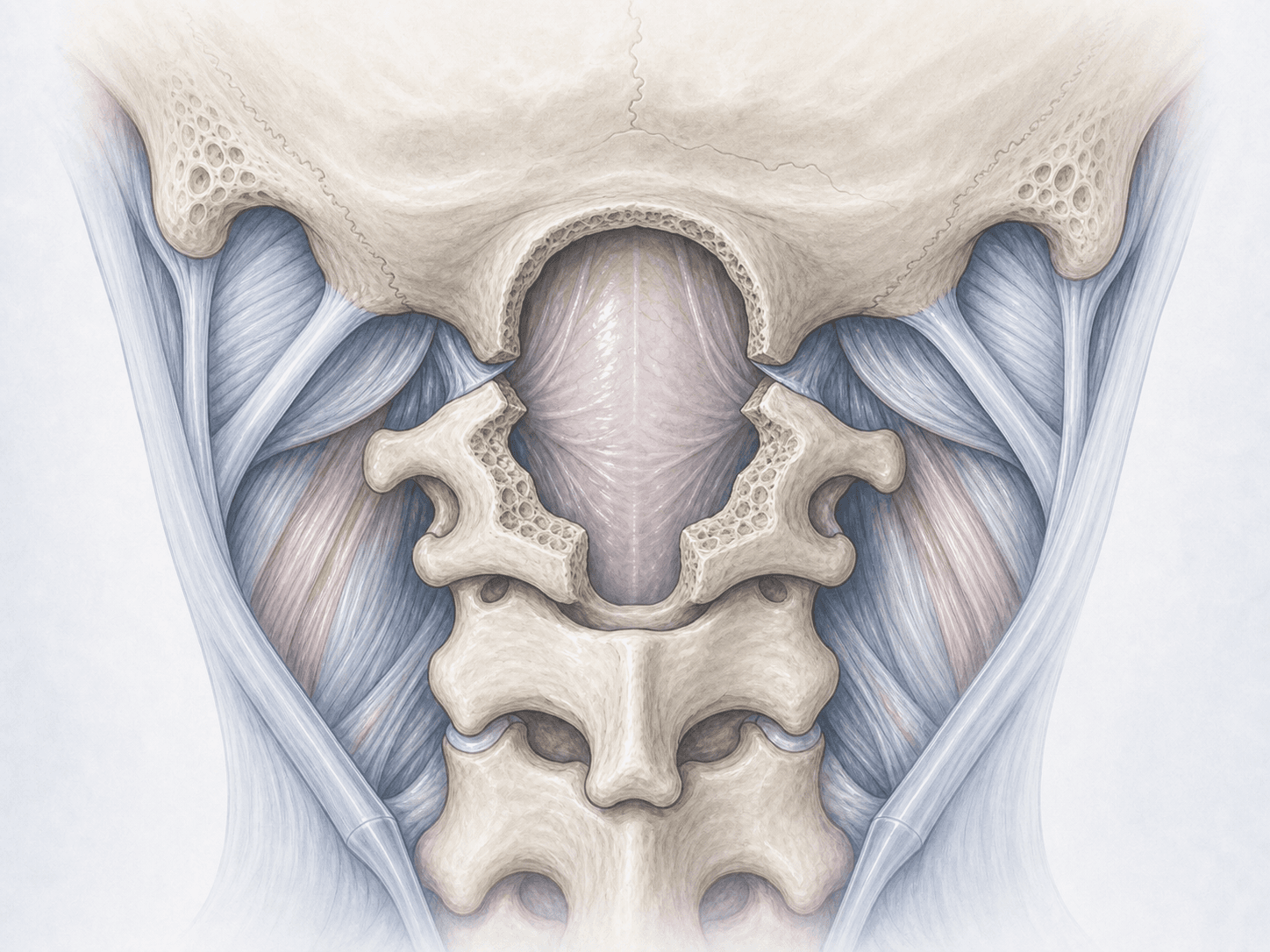
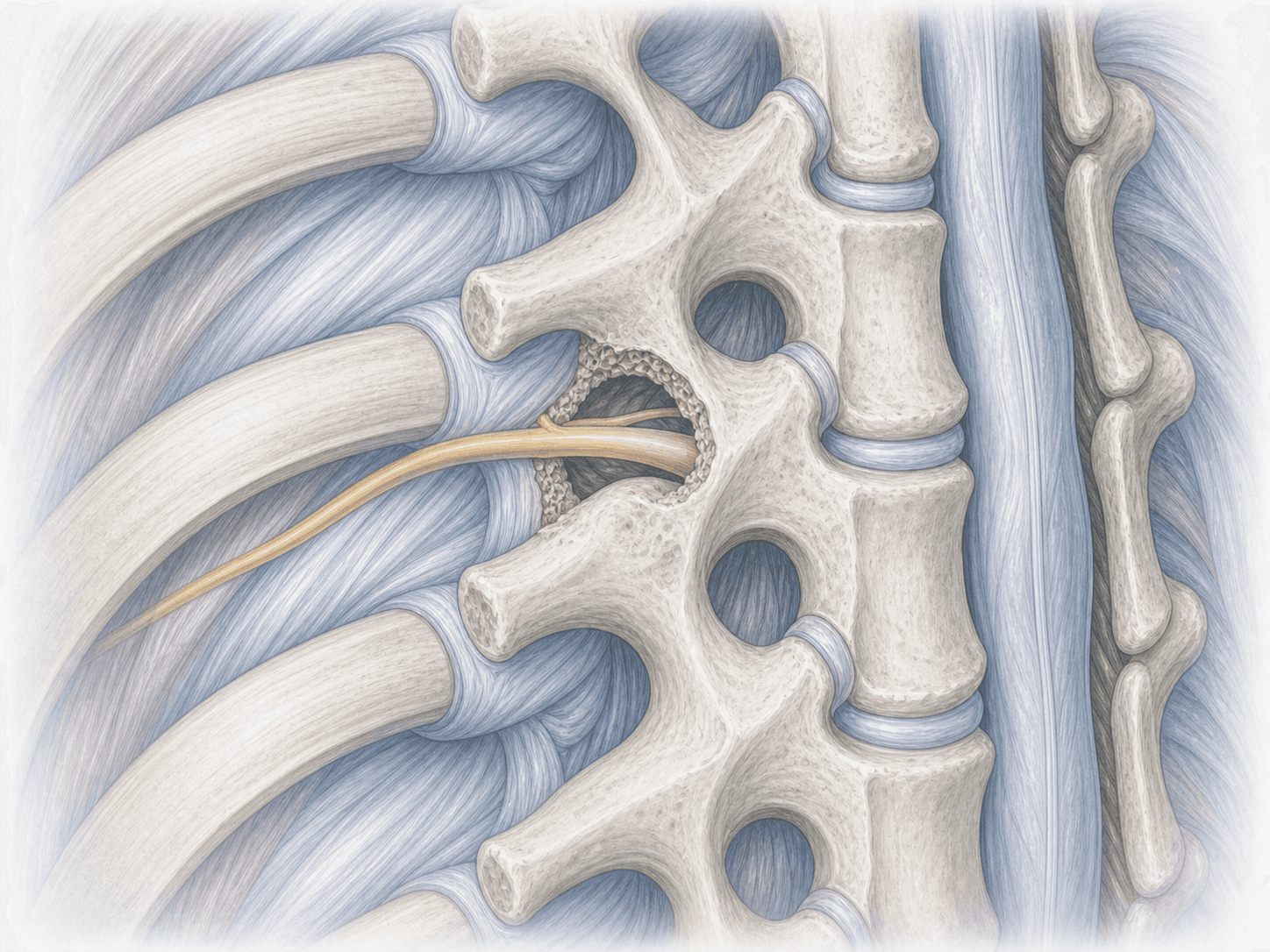
Cervical spine
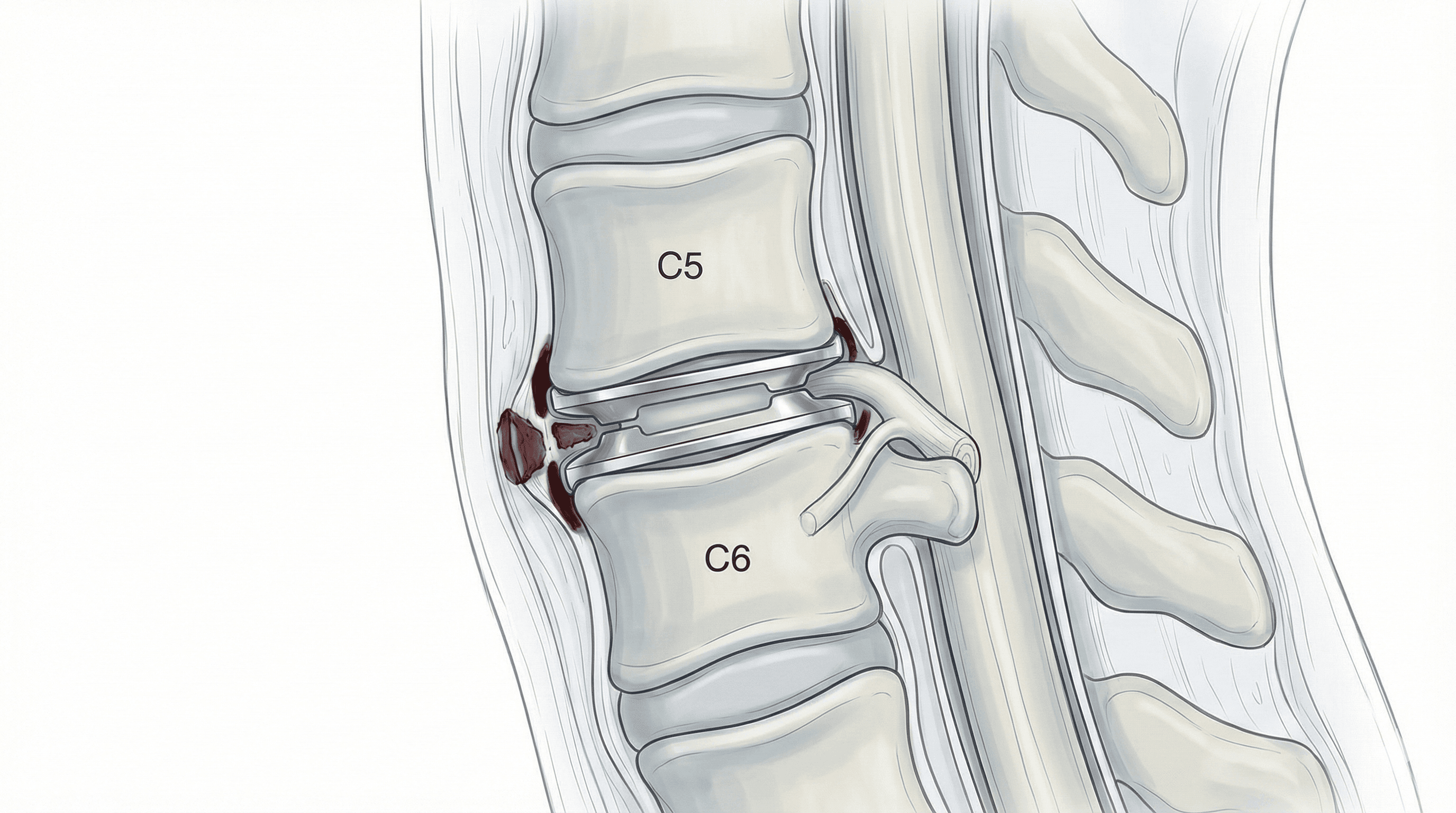
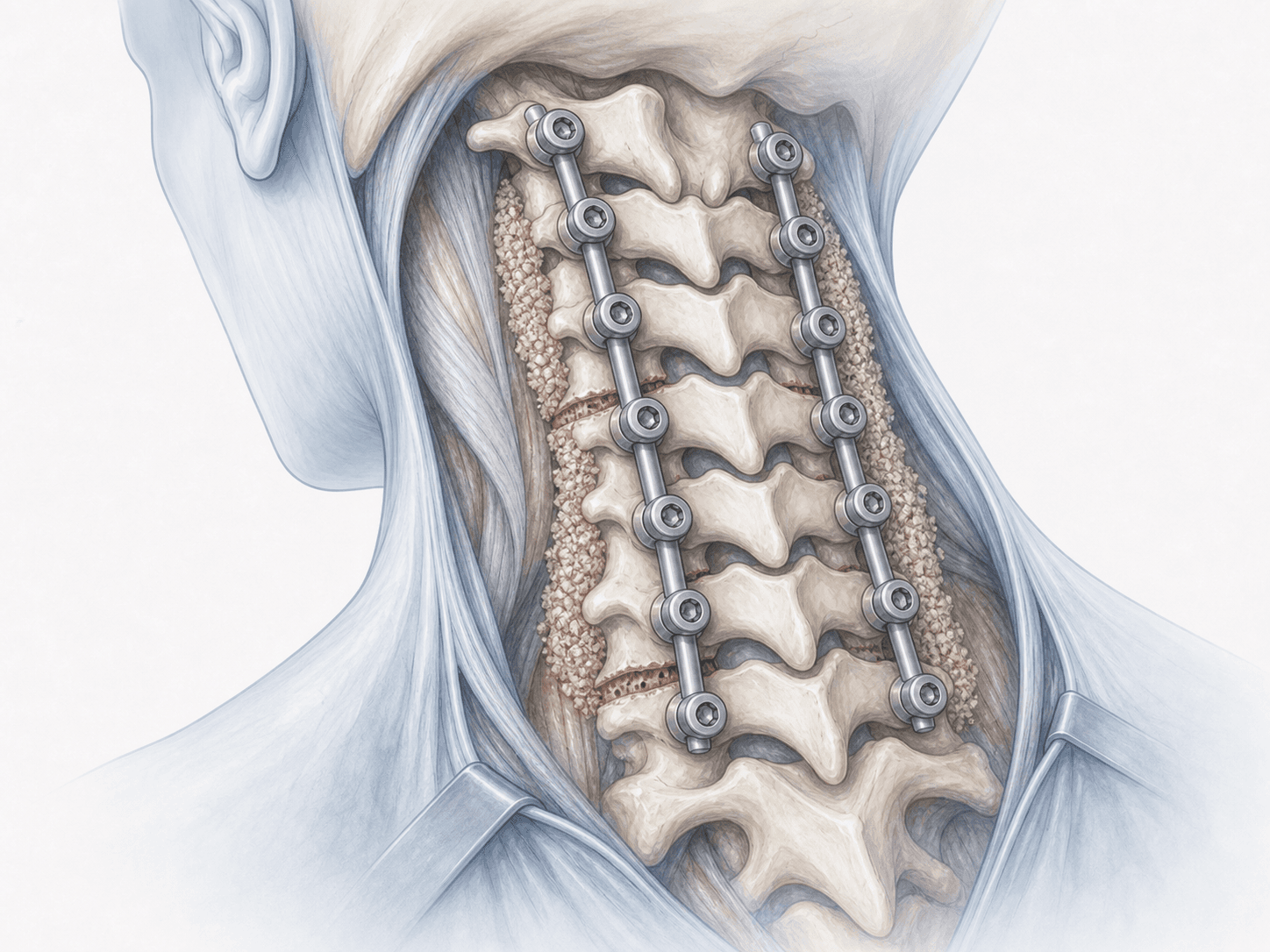
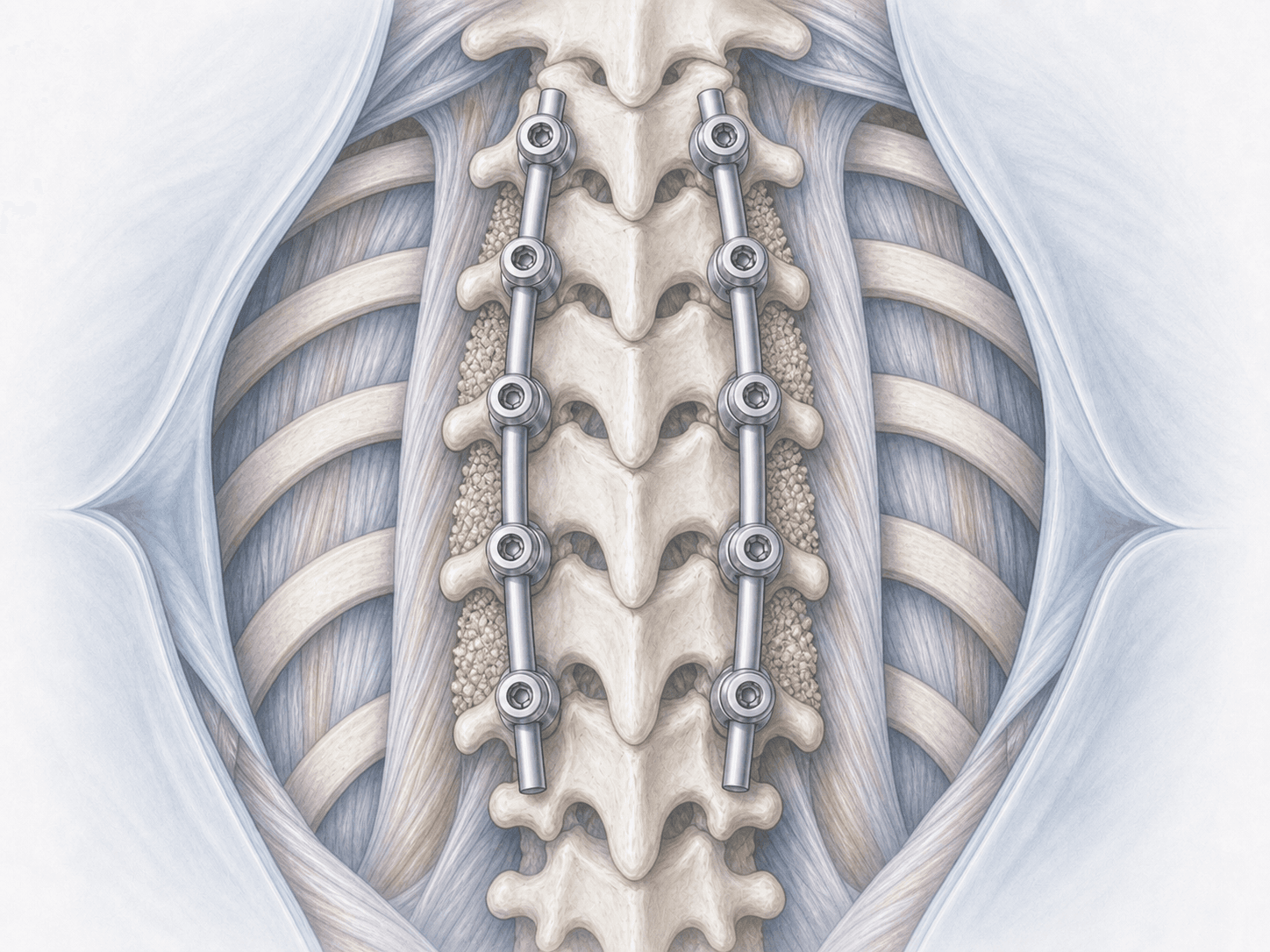
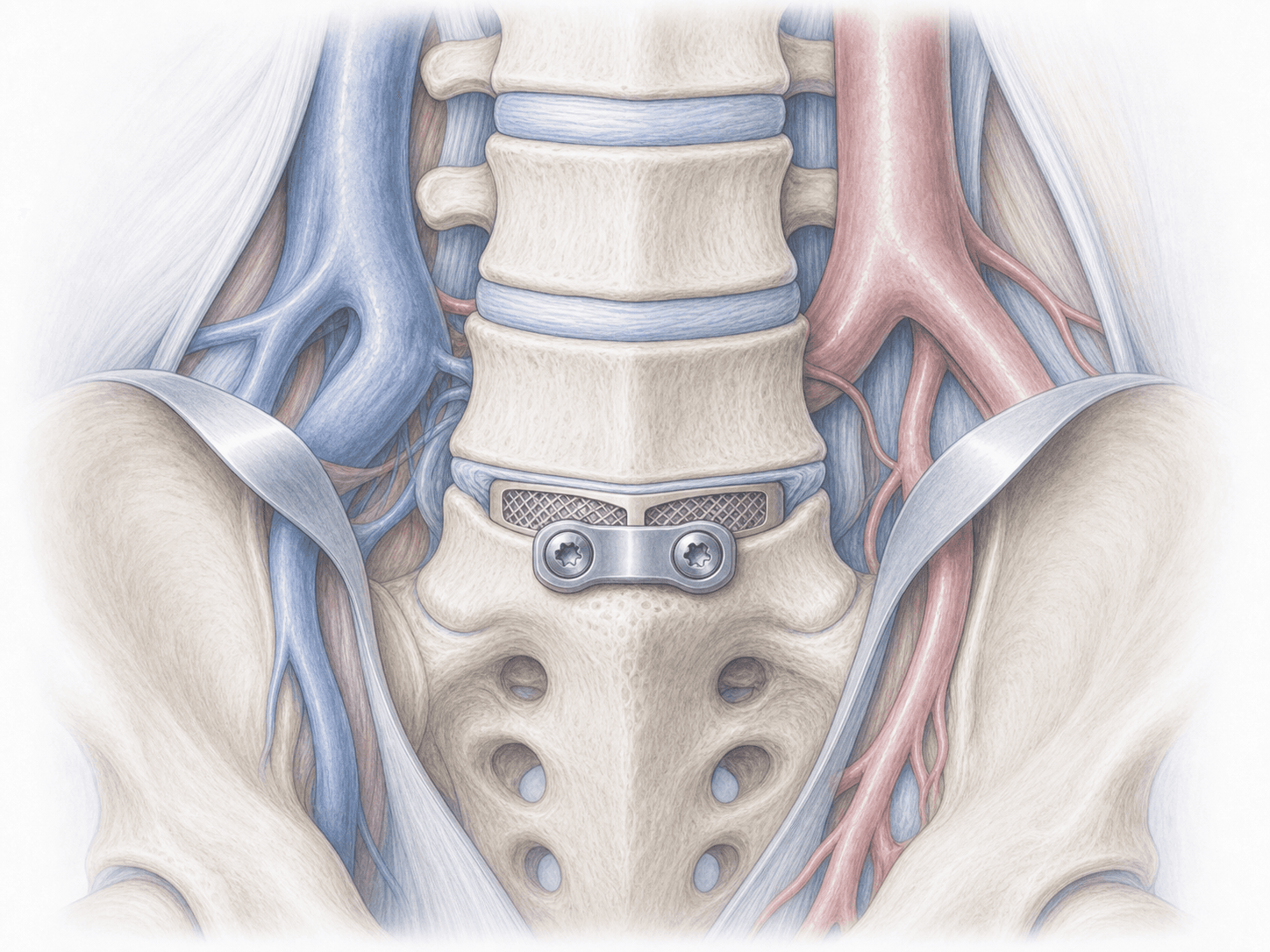
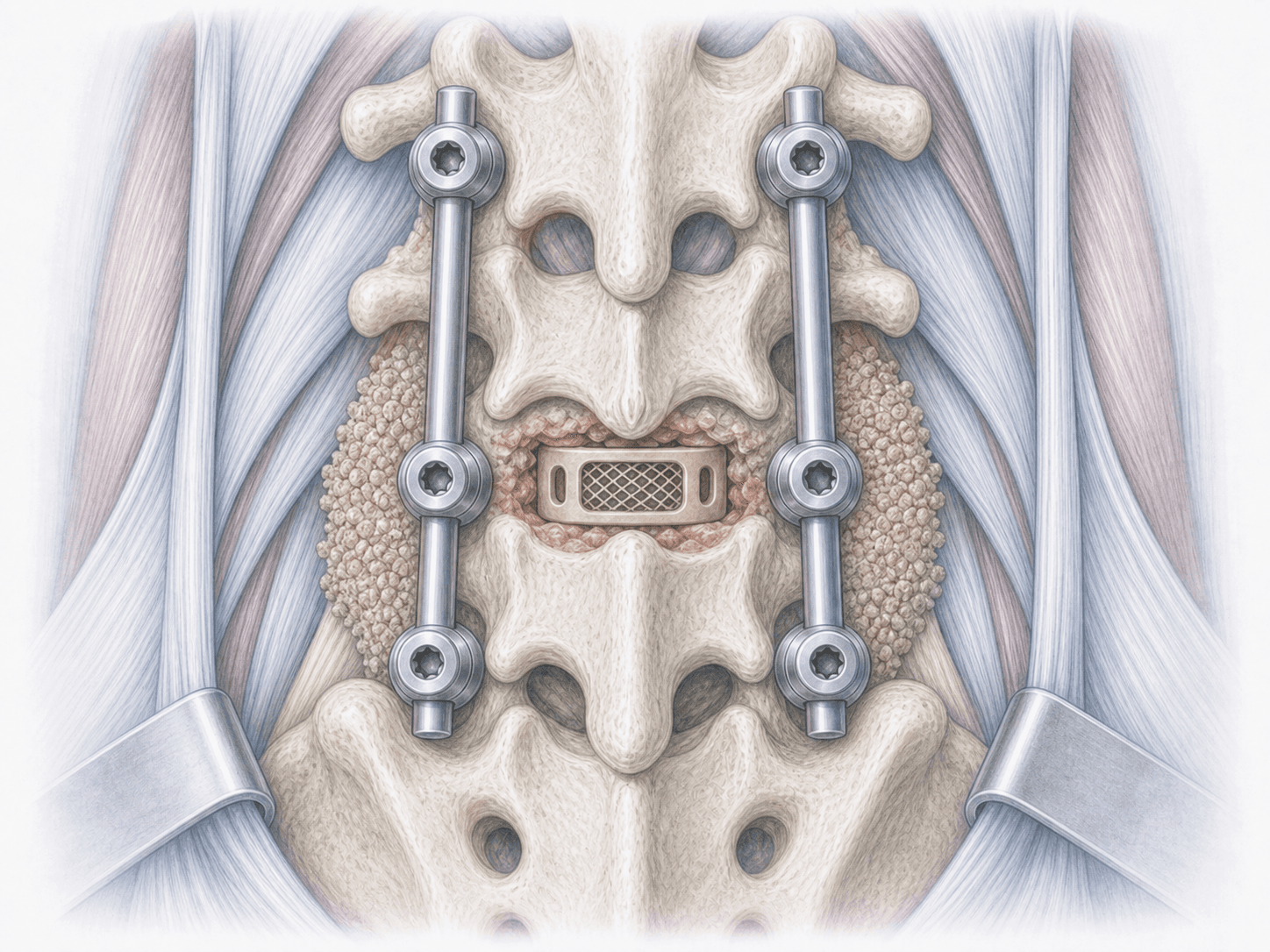
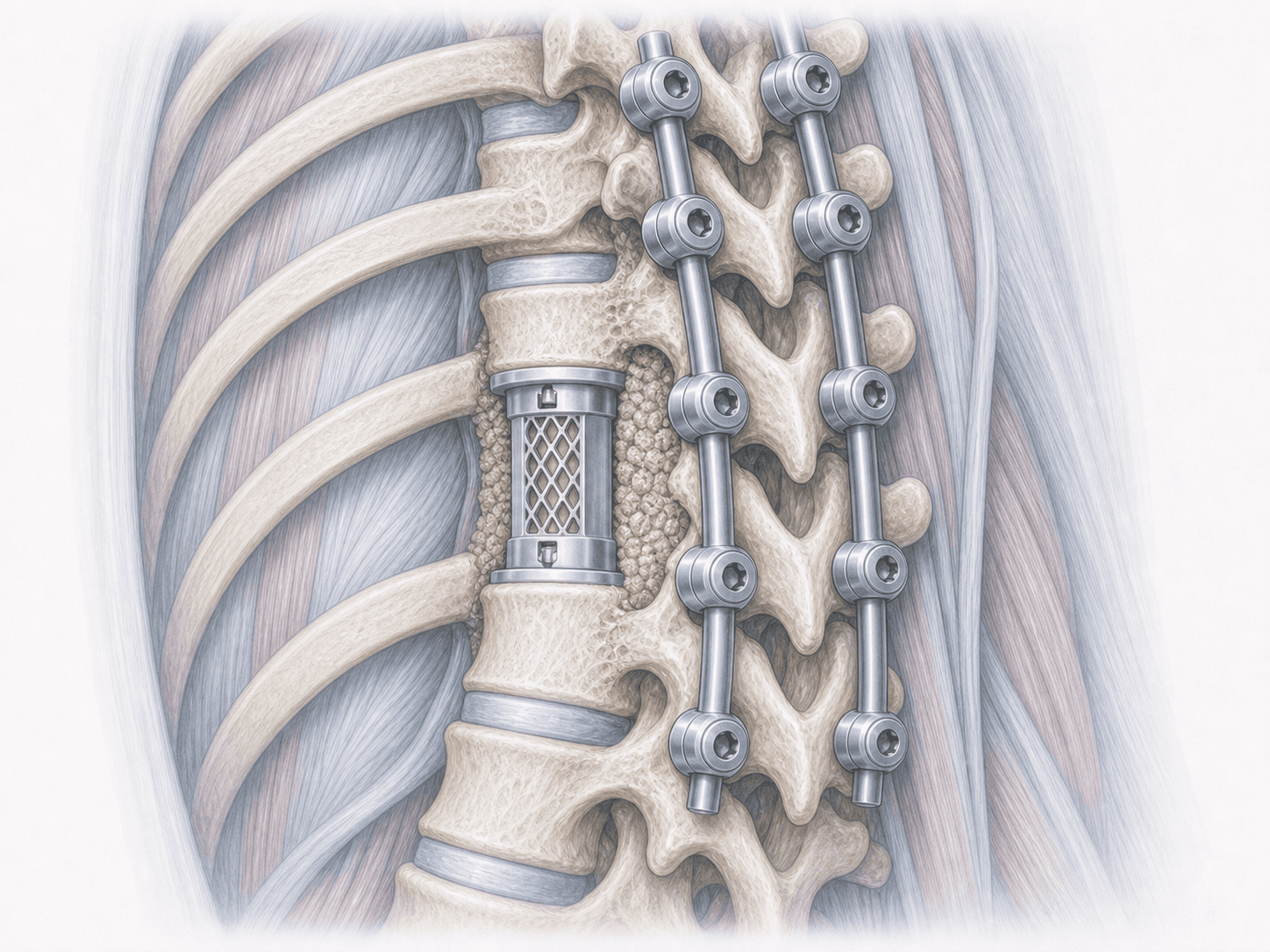
Anterior cervical fusion (interbody fusion with plate)
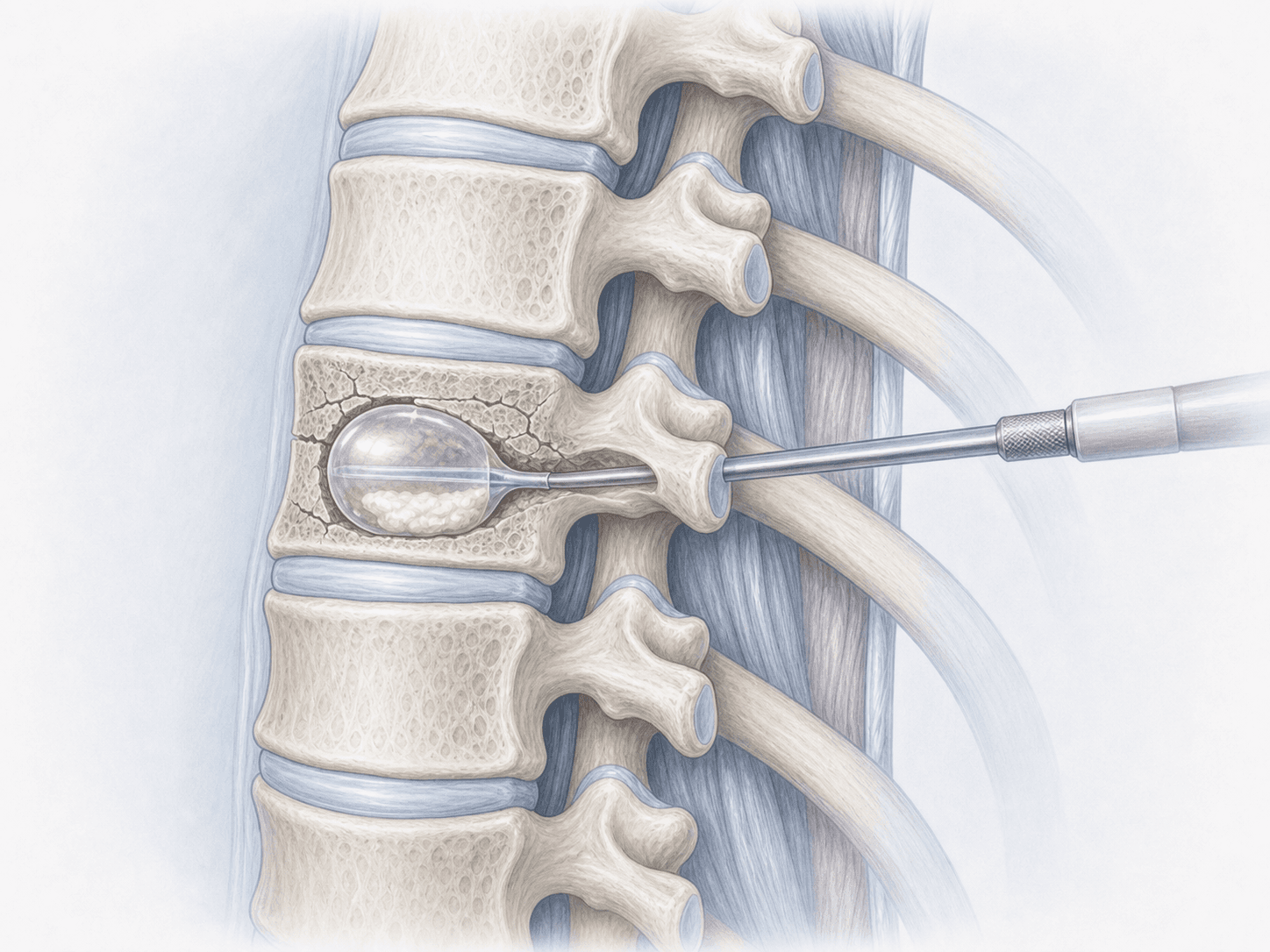
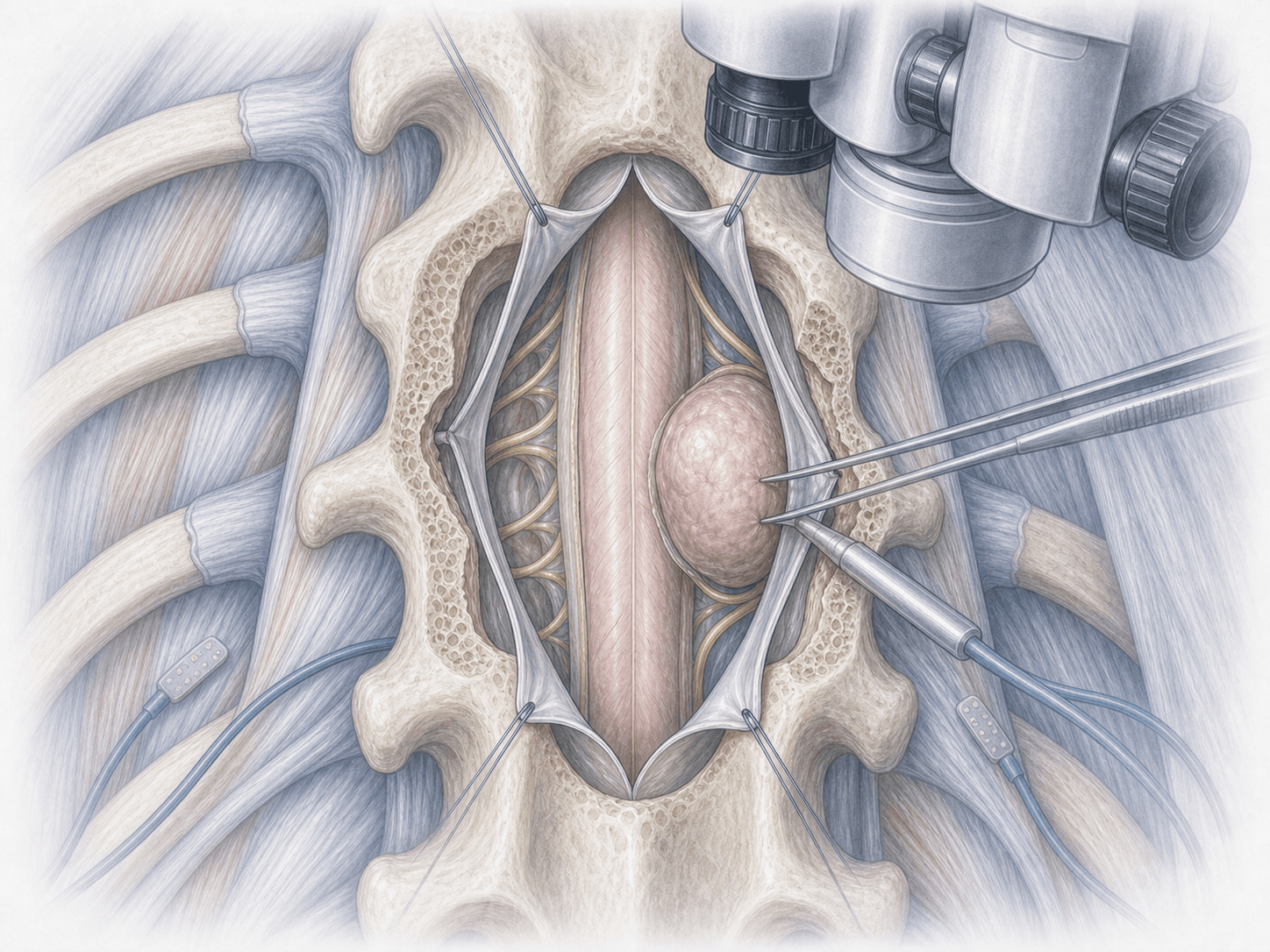
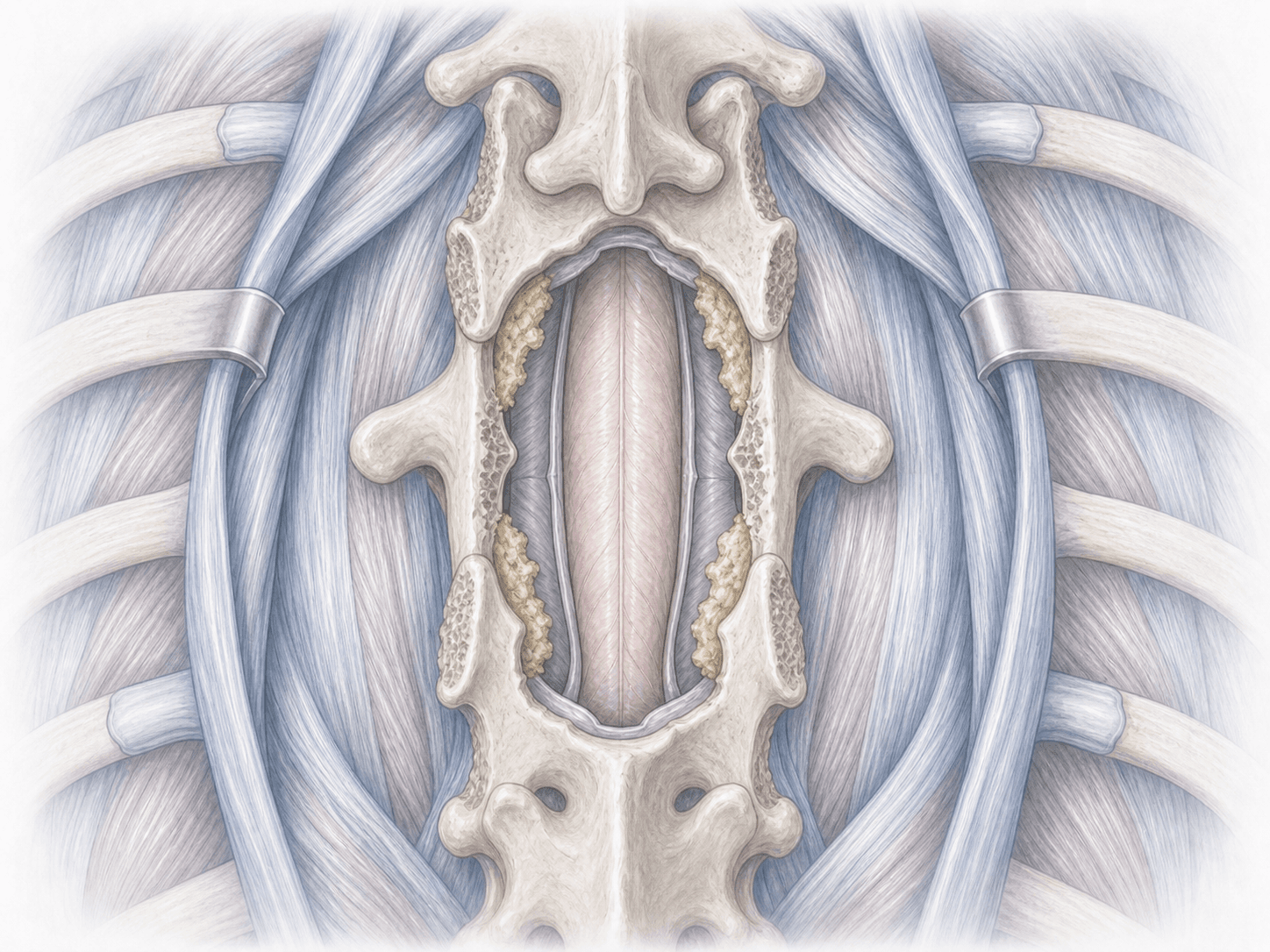
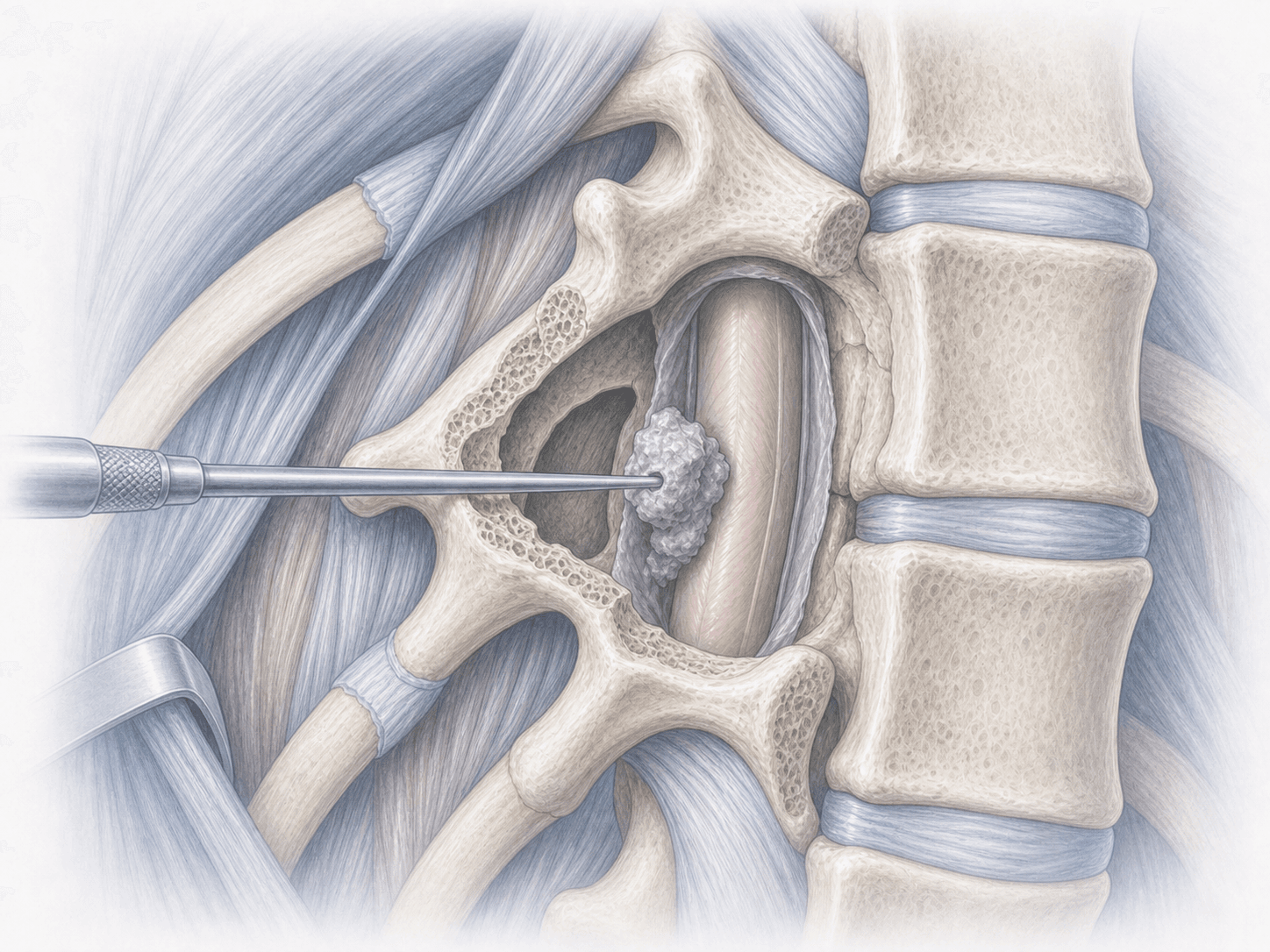
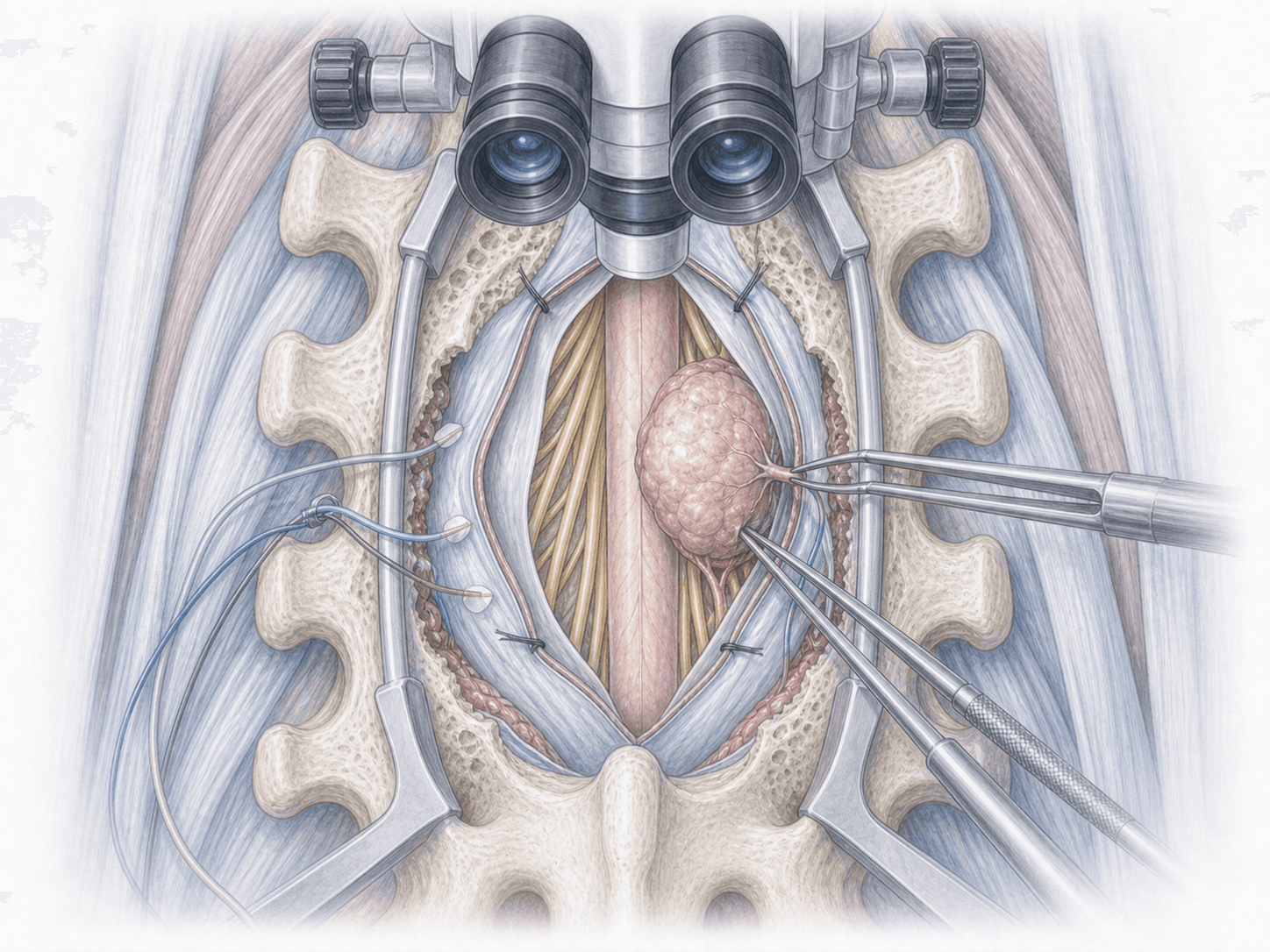
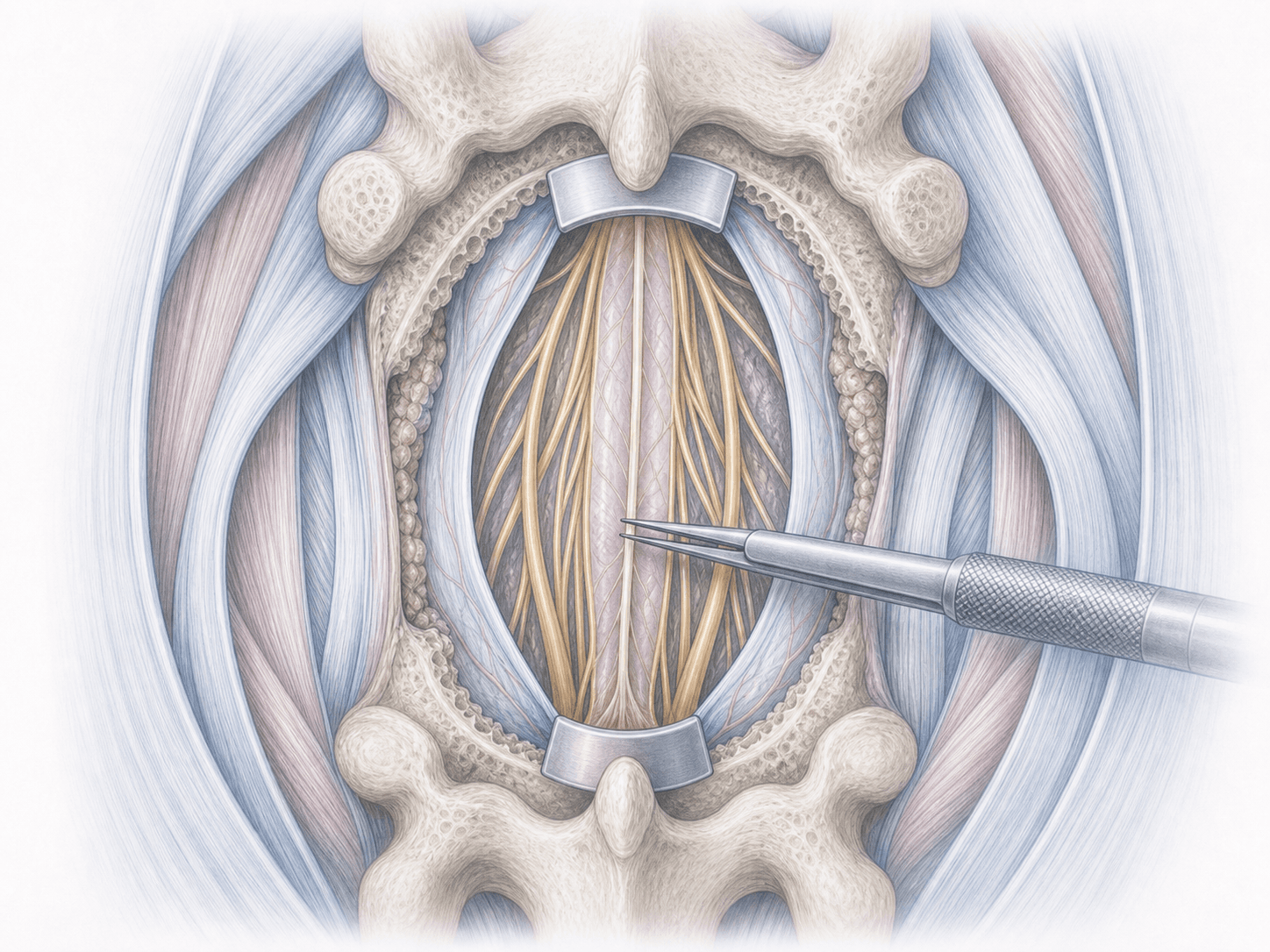
Anterior cervical surgery to decompress nerves and stabilise a severely degenerated or herniated disc when pain and symptoms persist despite medication, physiotherapy or injections.
View treatment