Primary vertebral tumour surgery
Primary vertebral tumour surgery treats bone tumours arising within the vertebra itself, both benign (symptomatic haemangioma, osteoid osteoma, aneurysmal bone cyst, eosinophilic granuloma) and malignant (chordoma, Ewing sarcoma, chondrosarcoma, osteosarcoma, multiple myeloma). Unlike metastatic disease, these tumours are uncommon and require careful planning by a multidisciplinary team involving neurosurgery, oncology, radiation oncology, pathology and interventional radiology. This guide explains in realistic terms when surgery is considered, how the type of resection is decided, what reconstruction is used and what to expect during recovery, accompanying you through a complex decision with the calm and clarity you deserve.
What is primary vertebral tumour surgery?
Primary vertebral tumour surgery involves resecting a bone tumour arising within the vertebra itself, together with the reconstruction and stabilisation needed to preserve spinal and spinal cord function. The strategy depends on whether the tumour is benign or malignant, where it sits within the vertebra and whether it extends into soft tissues or the spinal canal.
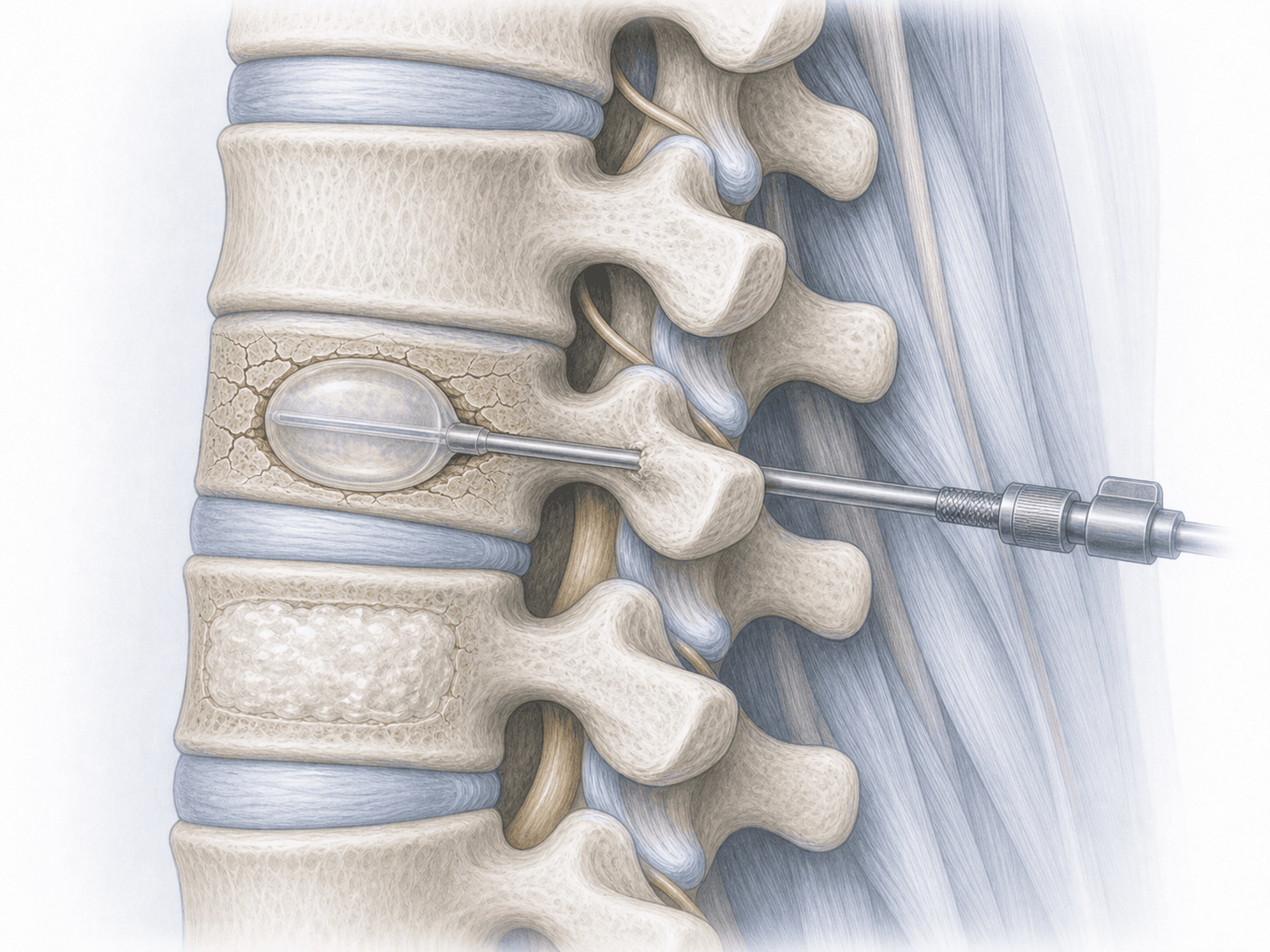
Planning relies on the Enneking classification (which considers the biological grade and the involved compartments) and, in the spine, on the Weinstein-Boriani-Biagini (WBB) classification, which divides the vertebra into zones to guide en bloc resection. In vascular tumours, such as many symptomatic haemangiomas, preoperative embolisation is performed to reduce blood loss. Unlike intraspinal tumours, which grow within the spinal canal, primary bone tumours frequently require vertebral body reconstruction with a cage, graft and/or posterior instrumentation. To discuss your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Primary vertebral tumours may remain silent for a long time or present with progressive symptoms:
When is this surgery indicated?
How is the procedure performed?
1.Preoperative preparation
Includes complete imaging (MRI, CT and sometimes PET-CT), preoperative biopsy when indicated and discussion at a multidisciplinary tumour board. The type of resection (intralesional, marginal or en bloc) is planned according to Enneking and WBB. In highly vascular tumours, such as symptomatic haemangiomas, preoperative embolisation is performed by interventional radiology. Medication and fasting are adjusted, and blood products are arranged.
2.During the procedure
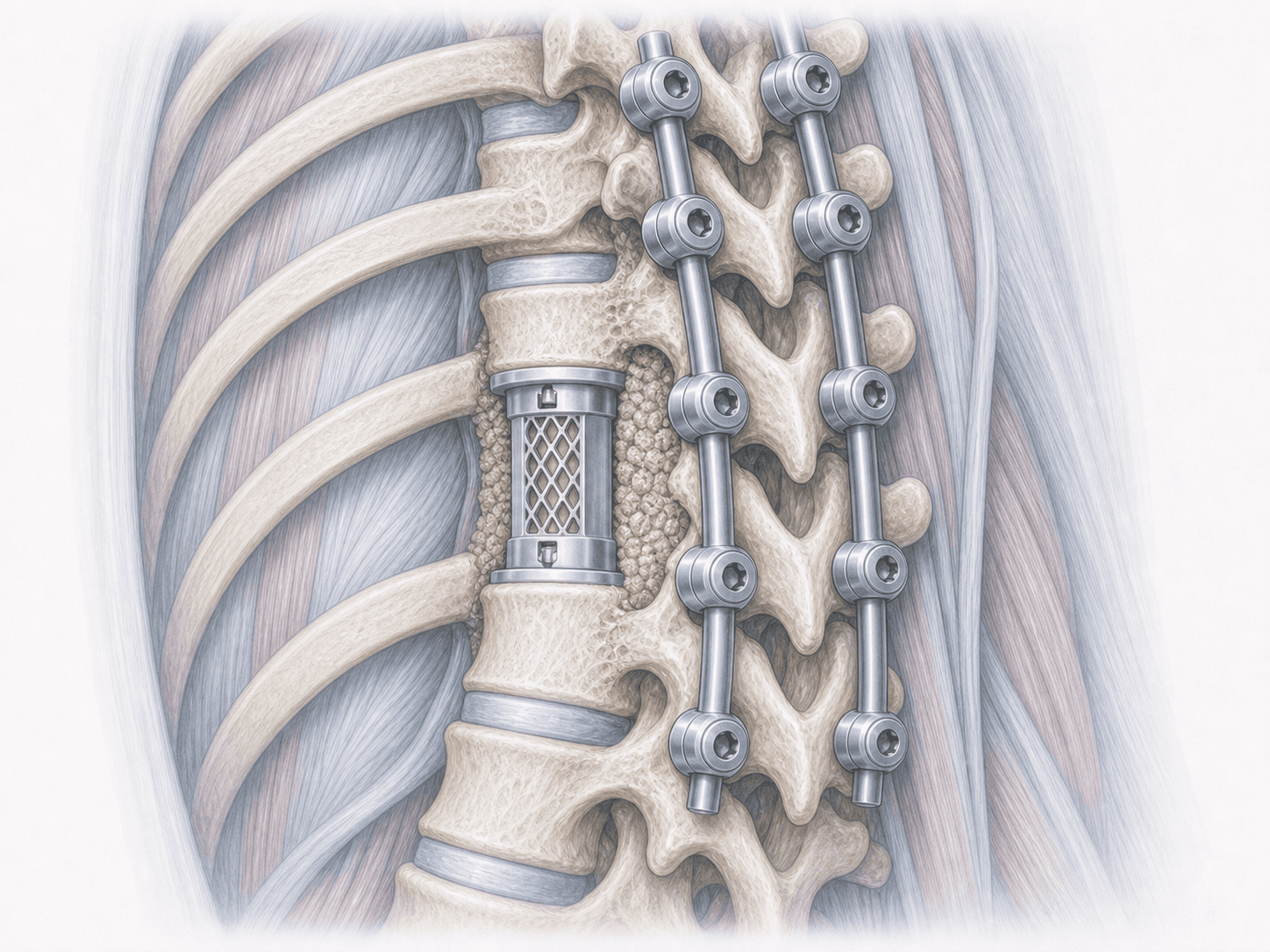
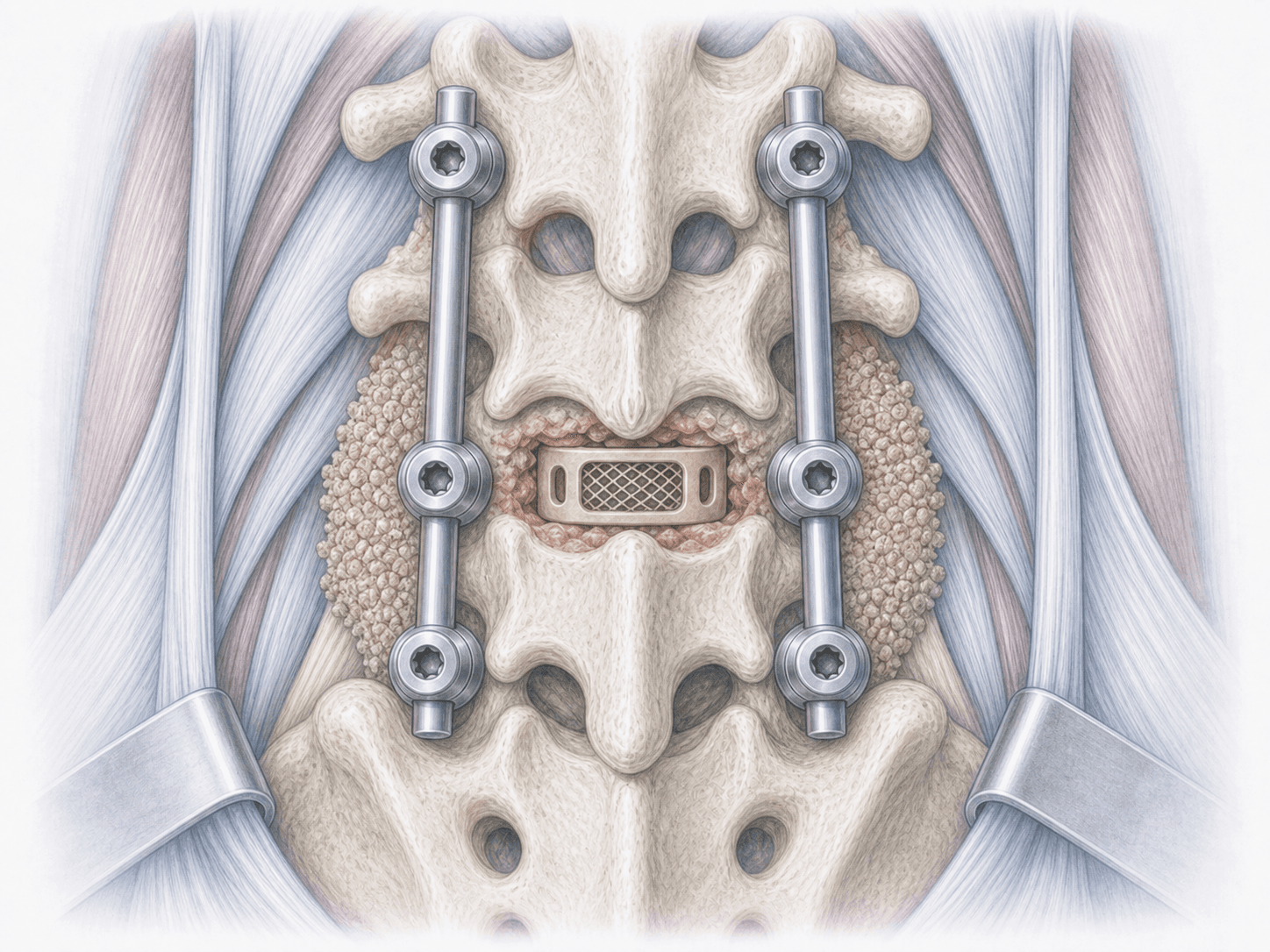
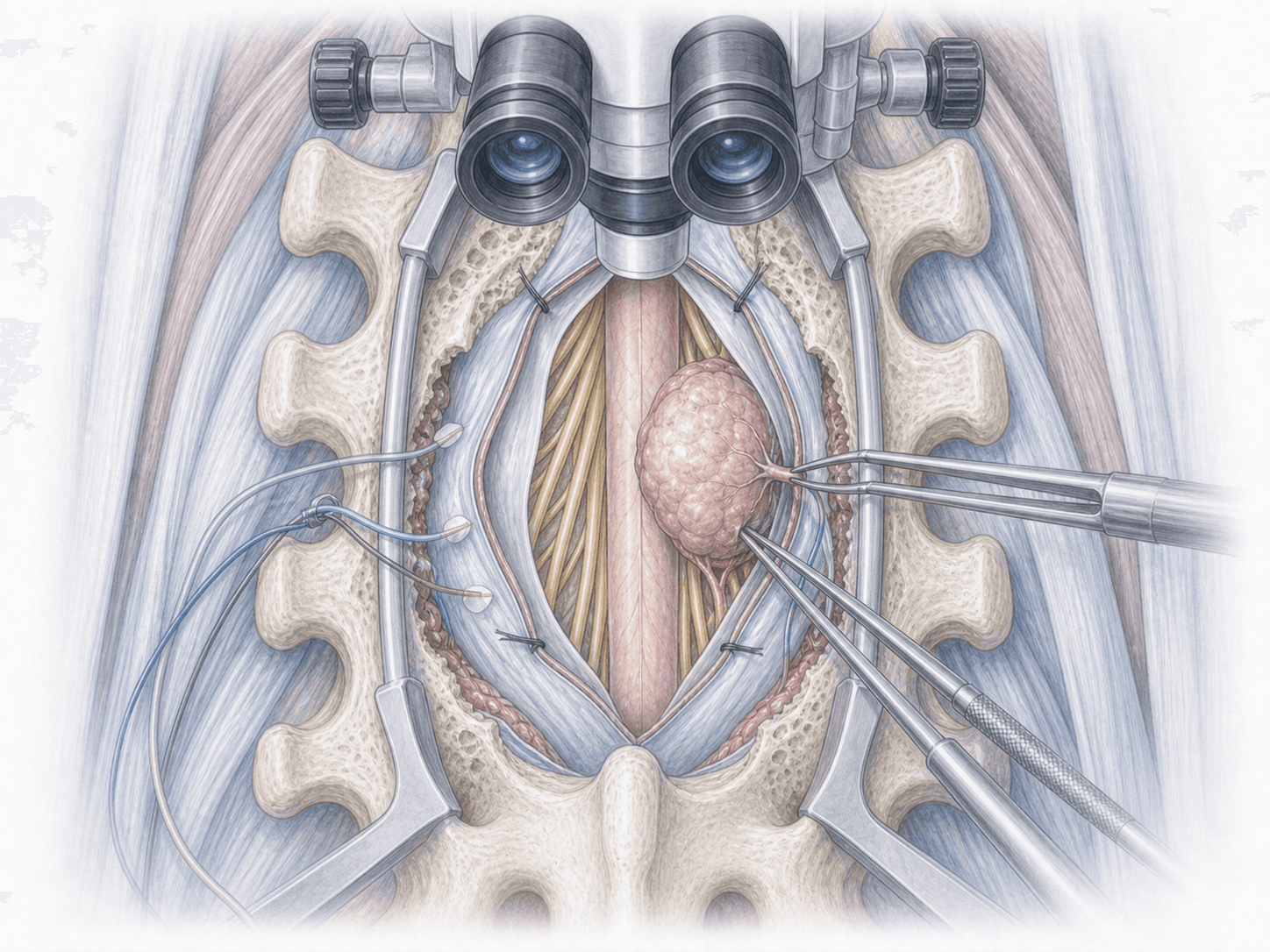
Under general anaesthesia and with intraoperative neuromonitoring, the vertebra is approached posteriorly, anteriorly or through a combined approach depending on the tumour location and the involved compartments. In potentially resectable malignant tumours, en bloc resection with oncological margins is attempted following WBB planning. In selected benign tumours, intralesional or marginal resection may be sufficient. After excision, the defect is reconstructed with an interbody cage, bone graft and/or cement, and the spine is stabilised with pedicle screws and rods.
3.Immediate postoperative period
Patients spend the first hours in an intermediate or intensive care unit depending on the extent of the resection. Pain, urine output, drain output and neurological function are monitored. Mobilisation usually begins within the first 24–72 hours with the rehabilitation team, sometimes with a brace or collar. Hospital stay ranges from a few days to 1–2 weeks depending on the type of surgery.
Recovery after primary vertebral tumour surgery
Recovery is gradual and depends on the type of tumour, the extent of the resection and any complementary treatments (chemotherapy or radiotherapy) decided by the multidisciplinary board. Return to daily activities usually takes from several weeks to a few months, with initial restrictions on loading and mobility.
Rehabilitation, nutritional support, psychological care and clinical and imaging follow-up are central to the process. Bone graft consolidation can take several months, so heavy strain is avoided early on. Fever, severe pain, new neurological deficit or wound problems require prompt medical review.
Risks and possible complications
All surgery carries general risks such as infection, bleeding, thrombosis or anaesthesia-related complications.
Specific risks of primary vertebral tumour surgery include spinal cord or nerve root injury, significant intraoperative bleeding (especially in vascular tumours), cerebrospinal fluid leak, wound healing problems, hardware loosening or failure, non-union of the bone graft (pseudarthrosis), local tumour recurrence and the need for complementary treatments such as radiotherapy or chemotherapy. Each risk is assessed individually before deciding the surgical plan.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala