Intraoperative neurophysiological monitoring
Intraoperative neurophysiological monitoring (IONM) is a safety technique that monitors the function of the spinal cord and nerves throughout surgery. Motor evoked potentials (MEP), somatosensory evoked potentials (SSEP) and electromyography (EMG) detect any change in real time, before it can become a permanent injury. Patients facing complex cervical surgery, spinal deformity correction, spinal cord decompression or tumour resection often ask what is done to protect the spinal cord and nerves during the procedure. IONM is part of that answer. This guide explains realistically what neurophysiological monitoring is, when it is used, how it unfolds during surgery and what it means when an intraoperative alert occurs.
What is intraoperative neurophysiological monitoring?
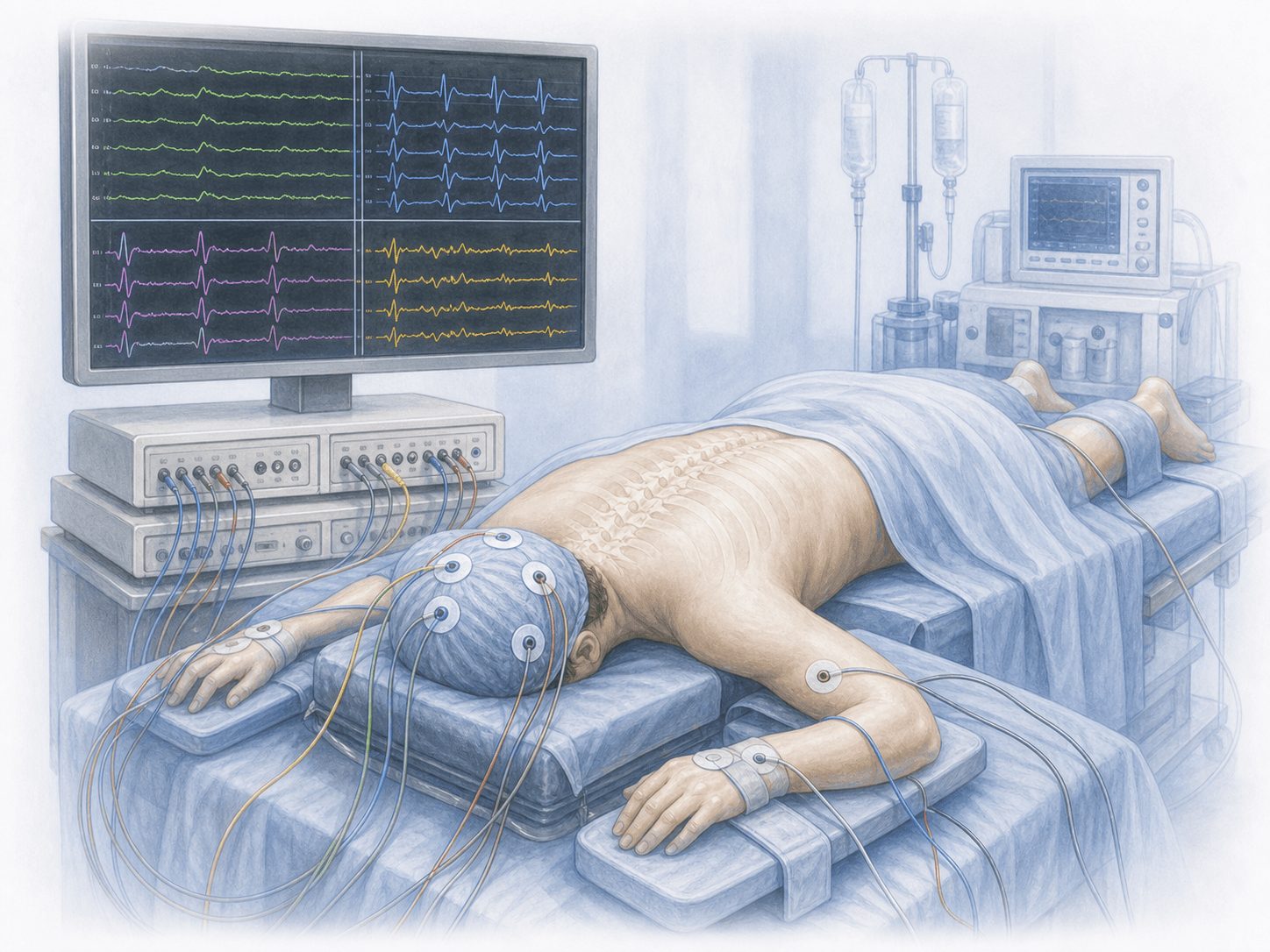
Intraoperative neurophysiological monitoring (IONM) is a set of techniques that record, in real time and throughout surgery, the function of the spinal cord, nerve roots and motor and sensory pathways. Three main tests are used: motor evoked potentials (MEP), which assess the integrity of the motor pathway; somatosensory evoked potentials (SSEP), which evaluate sensory pathways; and electromyography (EMG), spontaneous or triggered by stimulation, which detects irritation or contact with specific nerve roots.
IONM does not replace surgical judgement but acts as an early warning system: if a signal drops below an accepted threshold, the team can change the manoeuvre, release traction, review instrumentation or adapt the strategy before any permanent damage occurs. It is particularly useful in surgery with spinal cord involvement such as cervical myelopathy decompression, in deformity correction, intramedullary tumours and complex decompressions. To find out whether your surgery would benefit from monitoring, you can request an assessment with Dr. Ben Ghezala.
Which surgeries use monitoring?
IONM is considered standard in surgery with significant neurological risk. It is typically used, among others, in these situations:
When is monitoring indicated?
How is monitoring performed?
1.Preoperative preparation
Before surgery, the neurophysiologist reviews the patient's history, imaging and neurological examination to decide which modalities to use (MEP, SSEP, spontaneous EMG, triggered EMG) and where to place the electrodes. The anaesthetic protocol is agreed with the anaesthesiologist, since some drugs — particularly halogenated gases and muscle relaxants — can interfere with the signals. Total intravenous anaesthesia (TIVA) is usually preferred to preserve MEPs.
2.During the procedure
After anaesthetic induction, electrodes are placed on the scalp, target limb muscles and, depending on the case, in specific sites such as the anal sphincter or peripheral nerves. The neurophysiologist establishes a baseline before surgery starts and then monitors signals continuously. If a significant drop in amplitude or increase in latency crosses the alert thresholds, this is communicated immediately to the surgical team so the cause can be addressed: releasing traction, removing or repositioning an implant, adjusting blood pressure, waiting for signals to recover or changing the plan.
3.Immediate postoperative period
At the end of surgery a final check of the signals is performed to confirm a stable trace at closure. Electrodes are removed before awakening and, as soon as the patient is conscious, a basic neurological examination is carried out and compared with the preoperative one. The full monitoring record is included in the surgical report and forms part of the case documentation.
What it means for the patient's recovery
Monitoring itself does not add recovery time for the patient: electrodes are removed at the end of the procedure and, apart from small skin marks or minor discomfort at insertion sites, it leaves no lasting effects. The benefit is felt in overall safety: the patient wakes up knowing that the spinal cord and nerve roots were monitored throughout surgery and that, if any alert occurred, it was addressed before causing a deficit.
When an intraoperative change occurs and eventually recovers, that information also guides postoperative neurological follow-up. Rehabilitation, return to work and imaging follow-up follow the protocol of the main procedure (cervical, thoracic, lumbar or deformity surgery).
Limitations and possible drawbacks
Neurophysiological monitoring is very safe. Local drawbacks are minor: bruising or discomfort at electrode sites and, very rarely, tongue or lip bites caused by muscle contraction during MEPs (prevented with bite blocks).
From an interpretive standpoint, the technique is not infallible. False positives occur (signal drops without real injury, due to hypotension, hypothermia or anaesthetic effects), and false negatives are possible (injuries appearing without a clear alert, especially in non-monitored territories). IONM is therefore always interpreted within the clinical context, not as a standalone test. In addition, not every centre has the equipment and trained staff to use it routinely.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala