Thoracic spinal stenosis decompression
Thoracic spinal stenosis decompression is a surgery that releases the spinal cord in the dorsal spine when the canal has become narrow. The most frequent cause is hypertrophy or ossification of the ligamentum flavum, which compress the cord and trigger a progressive thoracic myelopathy with an unsteady gait. This guide explains when we consider surgery, how we perform it and what to expect during recovery, so you can decide calmly.
What is thoracic spinal stenosis decompression?
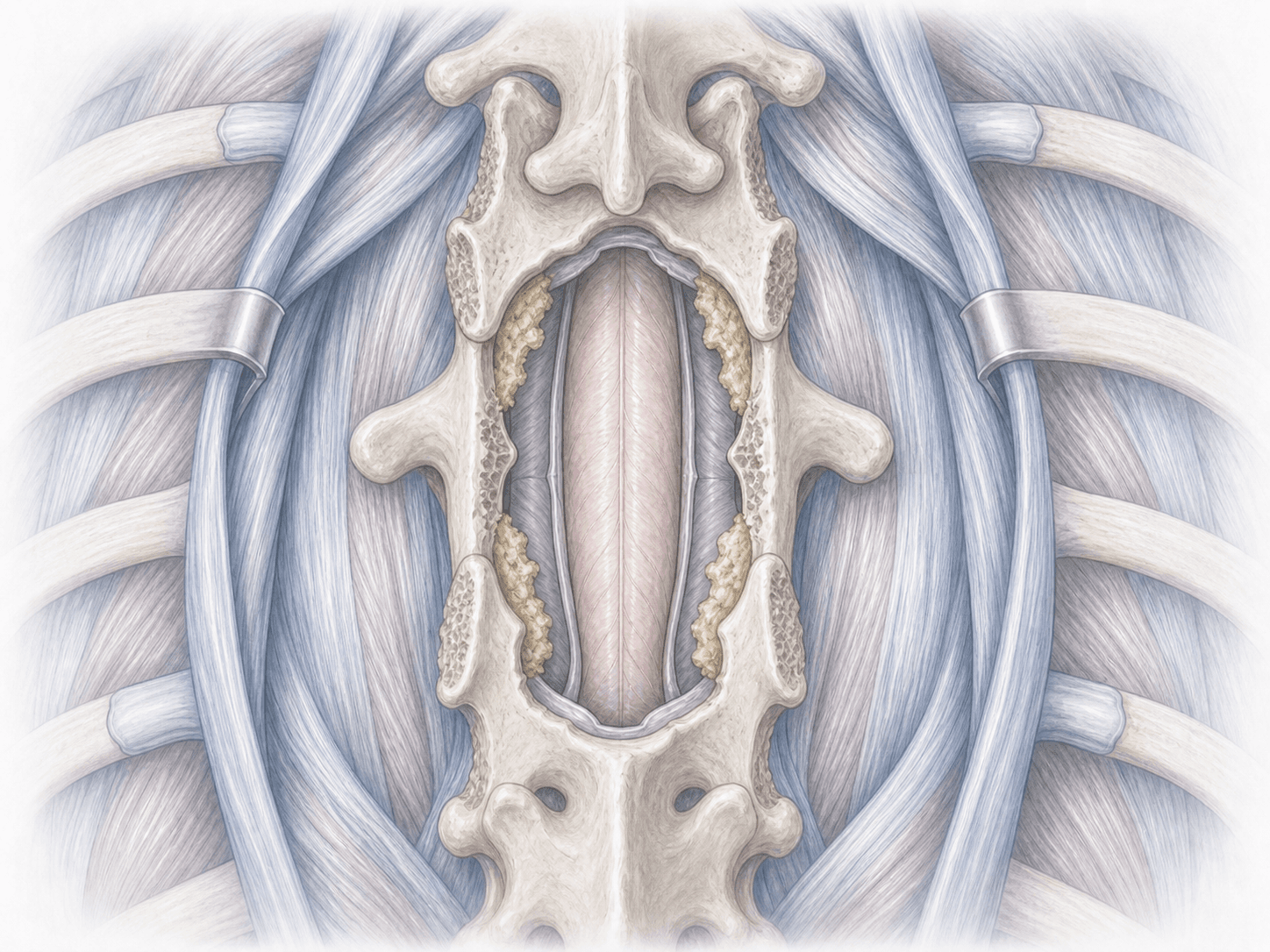
Thoracic spinal stenosis decompression is a surgery that releases the dorsal spinal cord when the canal has become narrow due to hypertrophy or ossification of the ligamentum flavum (OLF), facet arthritis or calcified disc herniations. The usual approach is posterior, through thoracic laminectomy and wide flavectomy, almost always with intraoperative neuromonitoring.
Unlike lumbar surgery, the thoracic cord is very sensitive and has little reserve, so the technique must be meticulous. To review your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients with thoracic stenosis typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
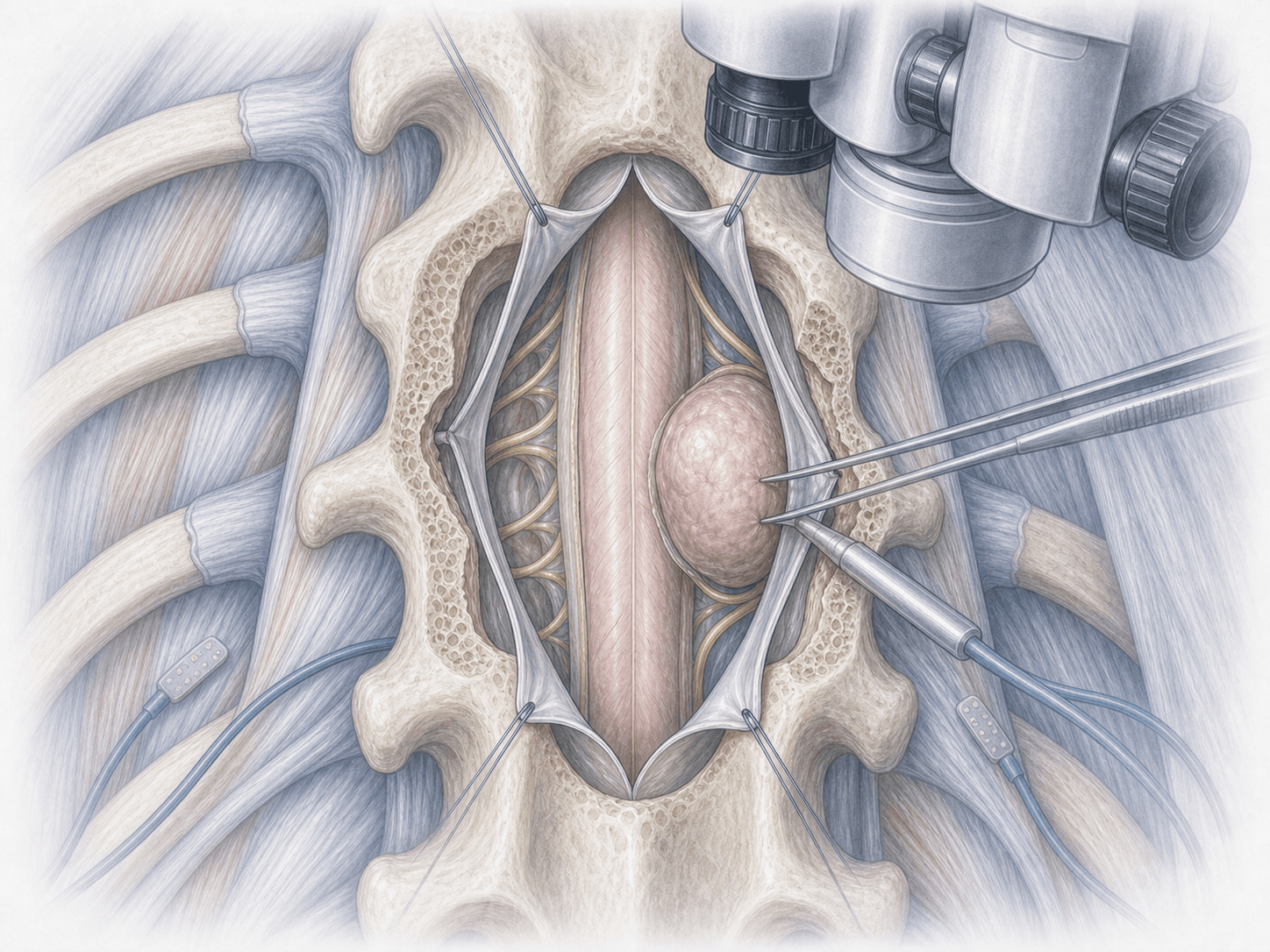
We review the MRI and CT to precisely locate the affected levels. Neurophysiological monitoring with motor (MEP) and somatosensory evoked potentials (SSEP) is planned. We provide fasting instructions, medication adjustments and tailored preoperative recommendations.
2.During the procedure
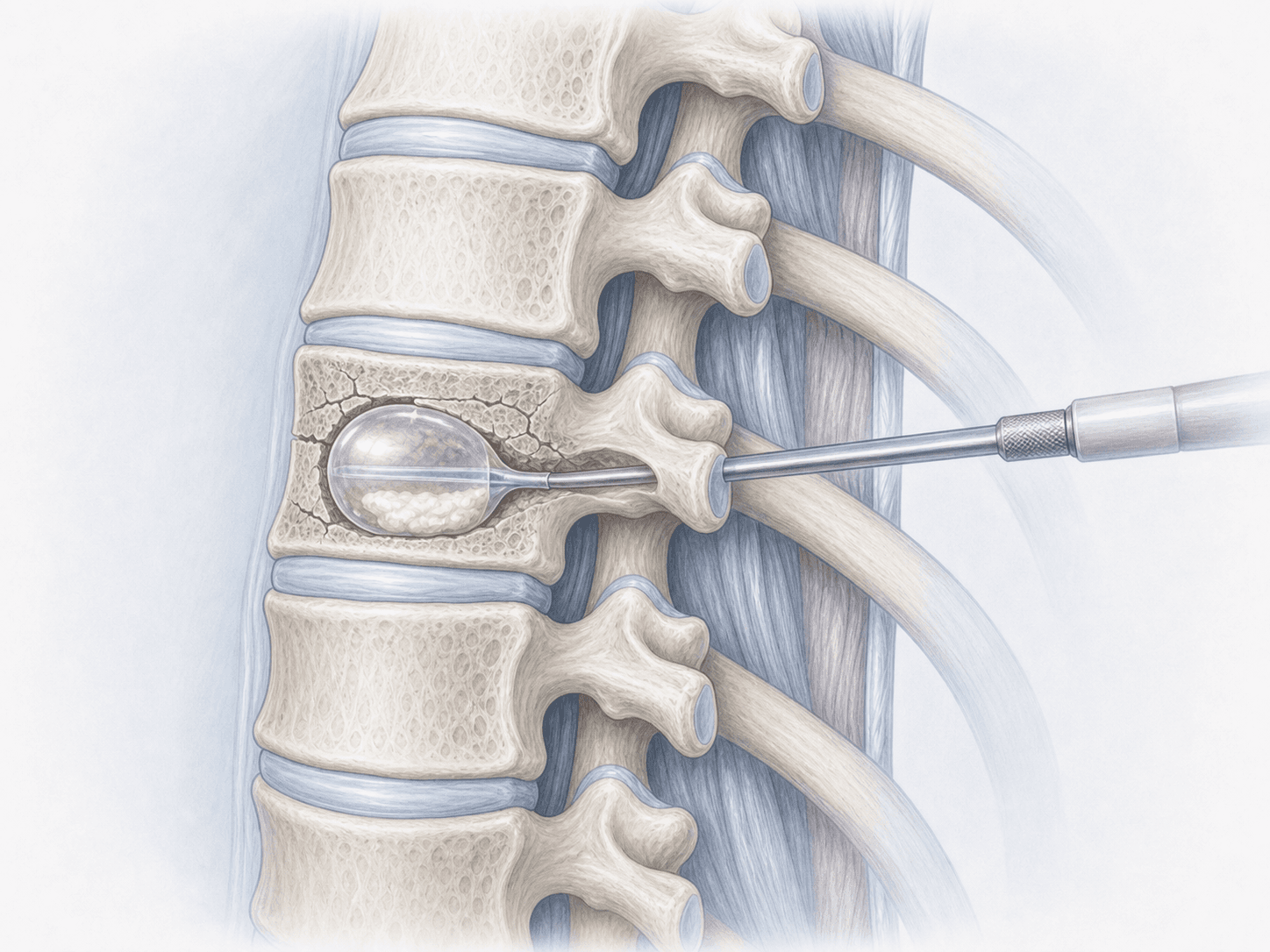
Surgery is performed prone under general anaesthesia with continuous neurophysiological monitoring. We use a posterior approach with laminectomy and wide flavectomy to release the cord without manipulating it. When the ossification adheres to the dura, we work under magnification with a floating-island technique to minimise neurological risk.
3.Immediate postoperative period
After surgery you spend a short time in recovery and return to your room. We monitor pain, neurological function and the wound. Sitting and assisted walking usually begin within 24–48 hours. Hospital stay is typically 3–5 days depending on clinical progress.
Recovery after thoracic decompression
Recovery is gradual and depends on how long the cord was compressed. Gait and balance often improve within the first weeks, while sensory changes and spasticity may take months.
We start early neurological rehabilitation focused on gait, balance and strength. Heavy strain and forced bending are avoided in the first weeks. Fever, new pain or loss of strength warrant prompt medical review.
Risks and possible complications
All surgery carries general risks such as infection, bleeding, anaesthesia-related issues and thrombosis.
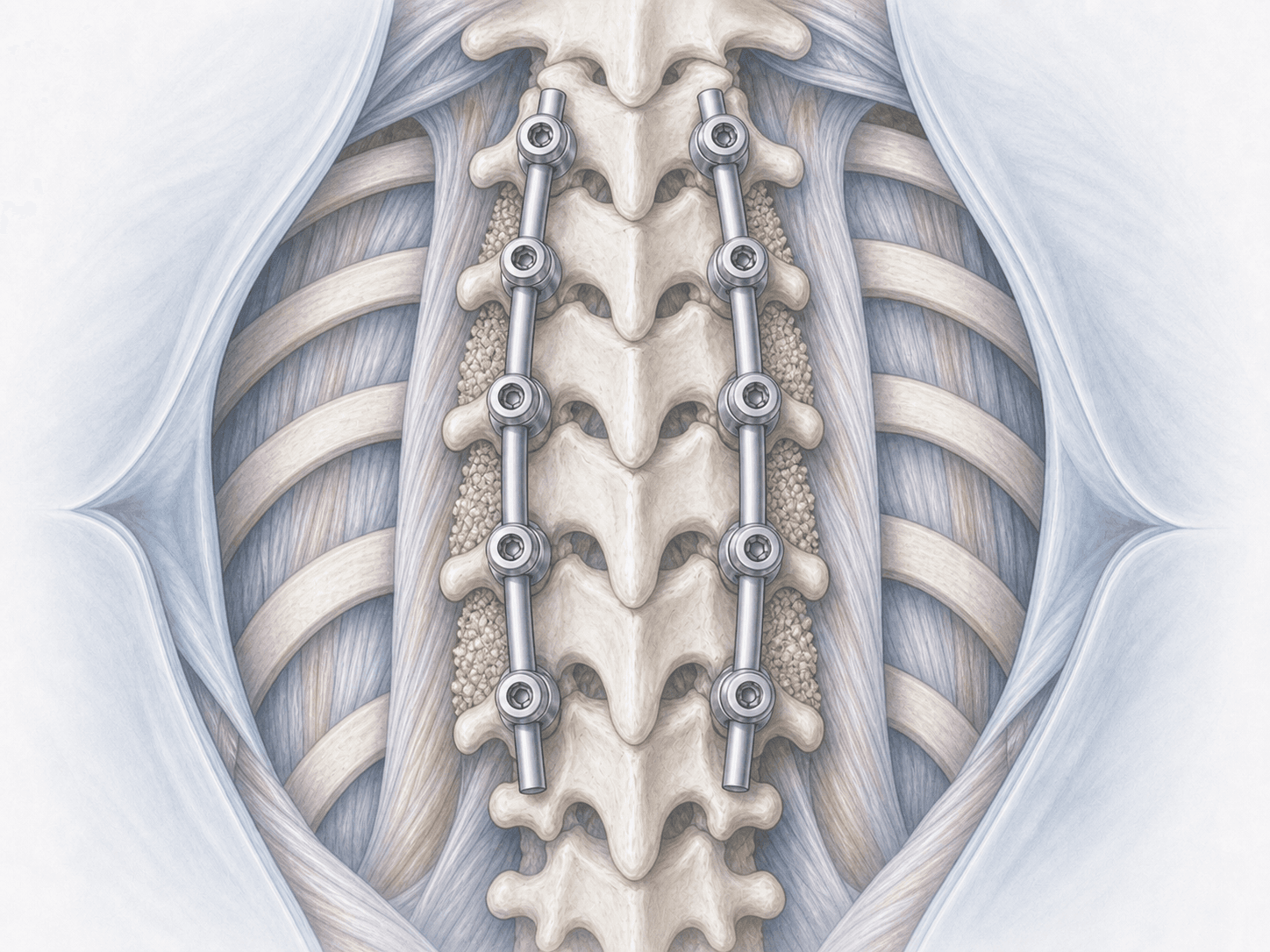
Specific risks of thoracic decompression include transient or permanent neurological worsening, cerebrospinal fluid leak (more likely when the ligament is ossified and adherent to the dura), segmental instability that may require fusion and, less often, recurrence of the stenosis. Each risk is assessed individually.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala