Filum terminale section for tethered cord
Filum terminale section is the operation that releases a tethered cord when the filum — the small ligament that anchors the tip of the spinal cord to the sacrum — is too tight or thickened and pulls the cord downward. Many adult patients reach our clinic in Alicante or Benidorm after years of atypical low back pain, tingling in the legs, a stretching sensation when bending or bowel and bladder problems that no conservative treatment has been able to ease. This guide honestly explains when we recommend surgery, what the technique involves, the role of neuromonitoring and why the indication in adults remains debated, so you can make a calm and fully informed decision.
What is filum terminale section?
Filum terminale section is an operation in which the filum terminale — the small fibrous ligament that anchors the lower end of the spinal cord to the sacrum — is cut to release a tethered cord. When that filum is too tight, thickened or contains fat, it keeps the spinal cord under tension, transmits traction to the lumbosacral roots and produces atypical low back pain, sensorimotor symptoms in the legs and bowel or bladder problems.
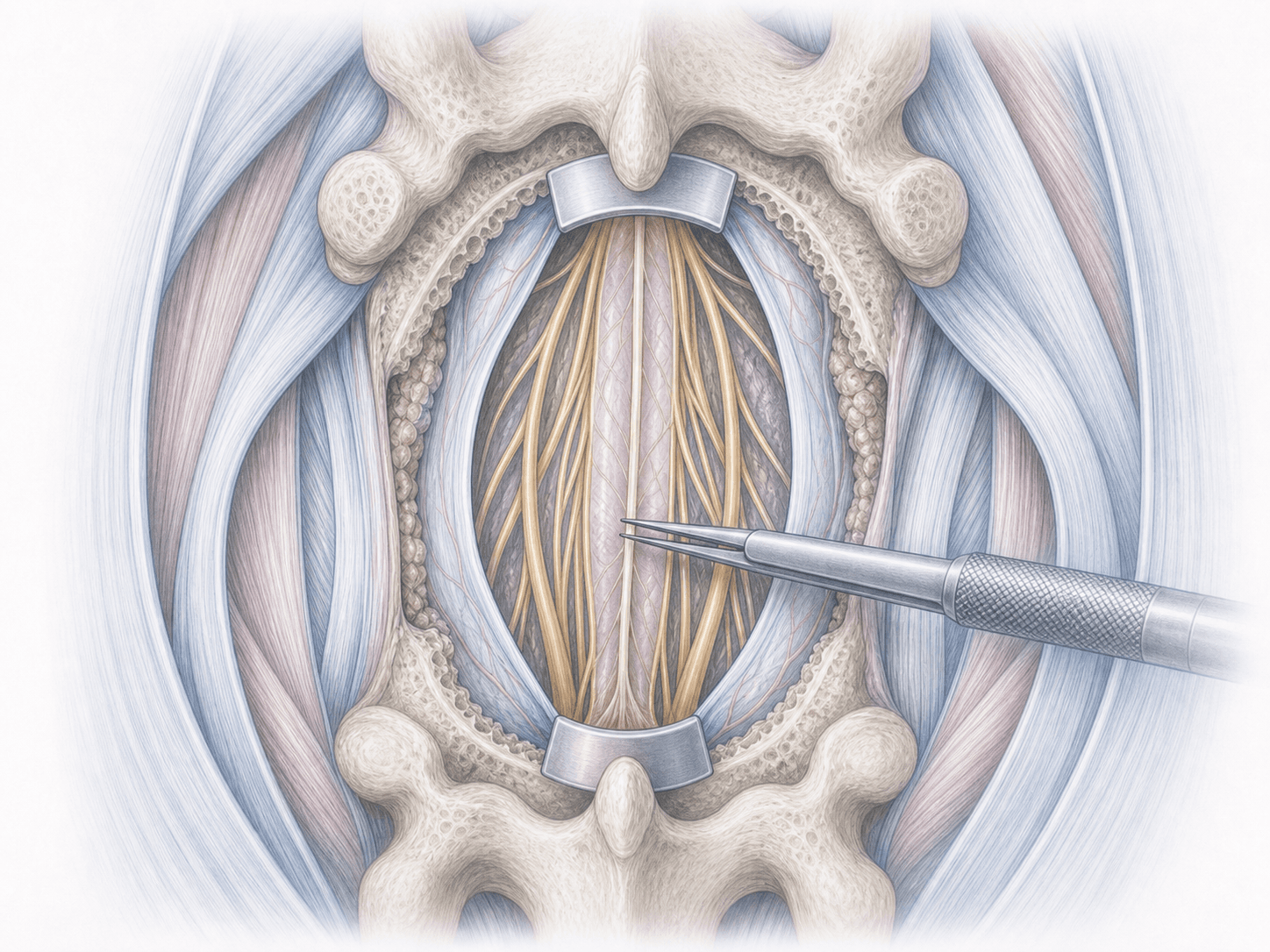
The procedure is performed through a posterior approach, with a small laminotomy between L5 and S1, careful opening of the dura, identification of the filum under the microscope and section under continuous neuromonitoring. Unlike other malformations of the neural axis such as Chiari I, no bony cranial decompression is performed here: the cord is freed from its most distal anchor. To discuss your case, you can request an assessment with Dr. Ben Ghezala in Alicante or Benidorm.
Symptoms and warning signs
Patients with a tethered cord from a tight filum terminale often report a mix of symptoms that have gone undiagnosed for years:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
Before surgery we review in detail the lumbosacral MRI, the urodynamic study when available and a full neurological examination. The procedure is explained, questions are addressed and tailored instructions are given for fasting, adjustment of anticoagulant medication and specific recommendations to reduce the risk of postoperative cerebrospinal fluid leak.
2.During the procedure
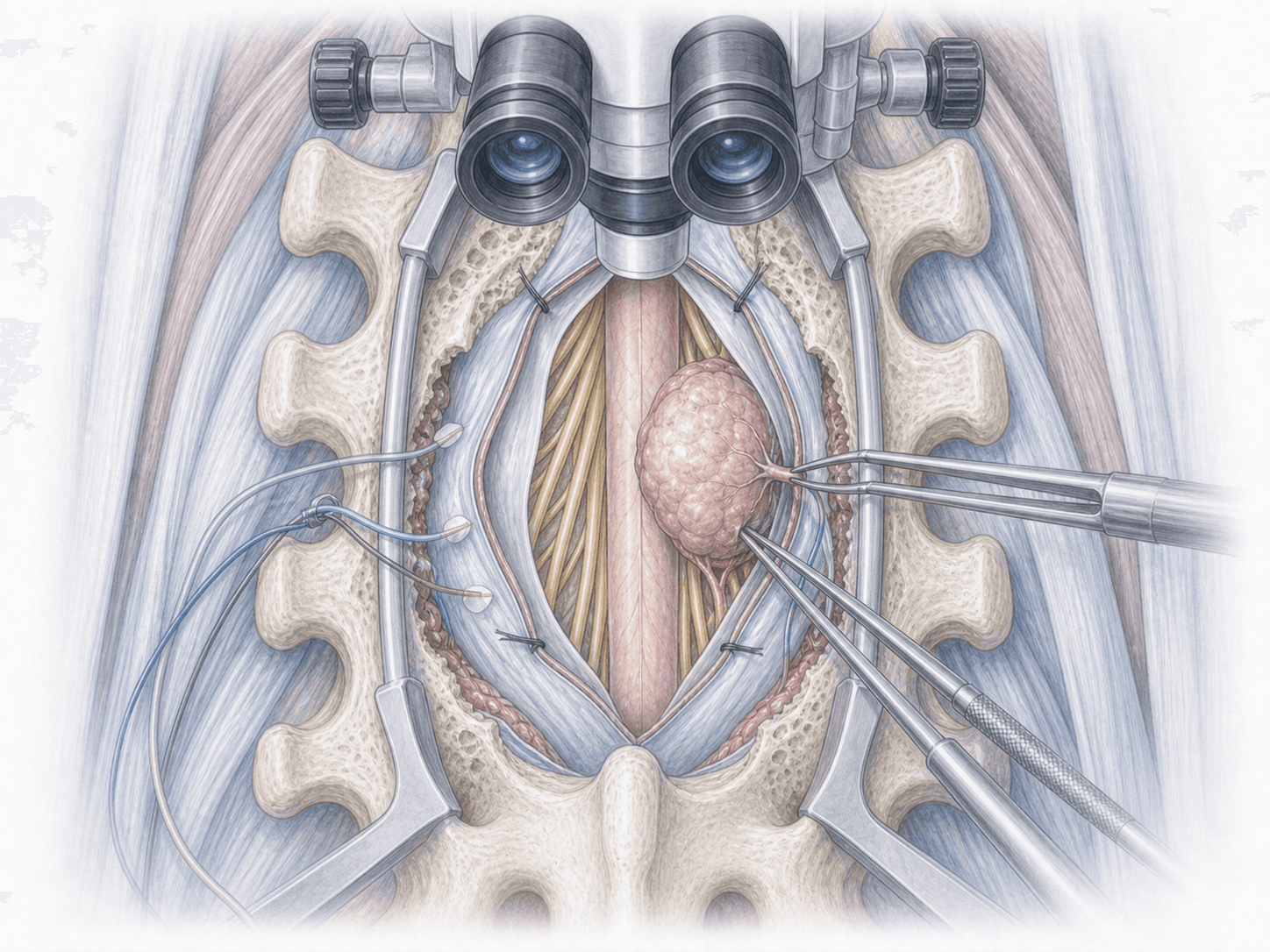
The patient is positioned prone under general anaesthesia with continuous intraoperative neuromonitoring (motor and sensory evoked potentials, EMG of sacral roots). A small laminotomy centred between L5 and S1 is performed, the dura is carefully opened and the filum terminale is identified, distinguished from nerve roots with the help of electrical stimulation. Once confirmed, the filum is divided, the released cord can be seen rising slightly, and the dura is closed in a watertight fashion with standard technique to minimise cerebrospinal fluid leak.
3.Immediate postoperative period
After surgery the patient spends a few hours in recovery before returning to the ward. Bed rest for 24–48 hours is maintained depending on progress, to reduce pressure on the dural closure and prevent cerebrospinal fluid leak. Pain is controlled, urine output and neurological examination are monitored and hospital stay is typically 3–5 days.
Recovery after filum terminale section
Recovery is gradual. Light daily activity is usually possible within one or two weeks, and office work is often resumed in 3–6 weeks. Physical jobs and heavier loads require more time and a tailored rehabilitation programme.
Improvement in low back pain and tingling tends to appear in the first few weeks, while bowel and bladder symptoms and strength take months to stabilise, as they depend on how long the cord had been tethered. Fever, severe orthostatic headache, fluid leaking from the wound or new neurological deficits warrant prompt medical review.
Risks and possible complications
All surgery carries general risks such as infection, bleeding, anaesthesia-related issues and thrombosis.
Specific risks of filum terminale section include cerebrospinal fluid leak and postoperative orthostatic headache, injury to lumbosacral roots with motor, sensory or sphincter consequences, deep infection or meningitis, haematoma at the surgical site and, in a proportion of adult patients, partial improvement or no response when the cord has been tethered for years. The controversy around occult tethered cord in adults makes it particularly important to weigh the individual risk-benefit balance before surgery.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala