Sacroiliac joint blocks
Sacroiliac joint blocks are an image-guided injection with a dual purpose: confirming that pain truly arises from that joint while simultaneously providing relief for weeks or months. Many patients arrive after months of unilateral buttock or low back pain that does not quite fit a disc herniation and that fails to improve with physiotherapy or anti-inflammatories. The sacroiliac joint accounts for roughly 15–30% of low back pain cases and is easily missed. This guide explains when a block is indicated, how it is performed and what information it provides to plan the next step.
What is a sacroiliac joint block?
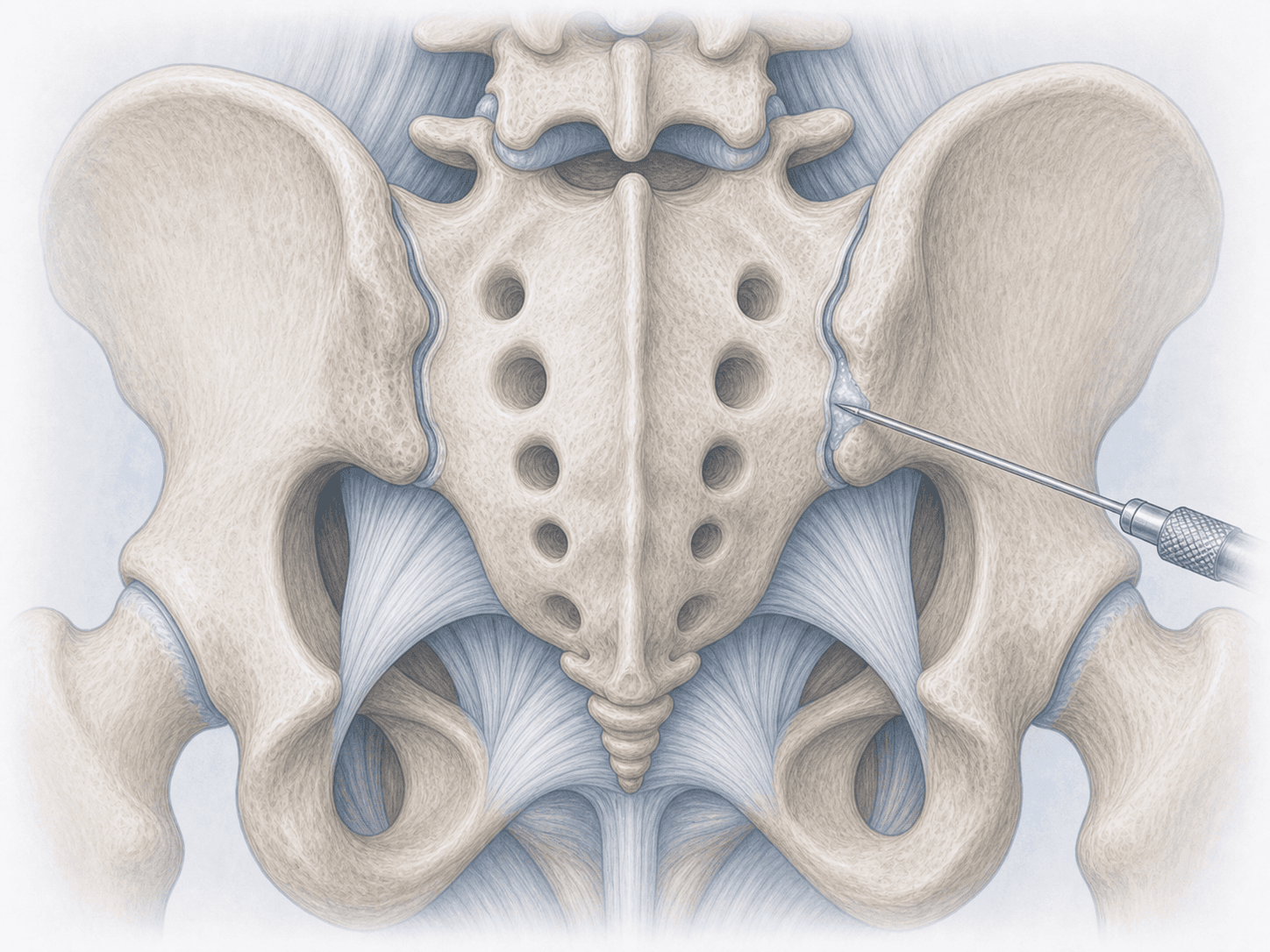
A sacroiliac joint block is an intra-articular injection in which a small dose of local anaesthetic and a long-acting corticosteroid are delivered into the joint under fluoroscopic or ultrasound guidance. It serves both as a diagnostic test (if pain disappears within the first hours, the joint is confirmed as the source) and as a treatment (the steroid reduces inflammation for weeks or months).
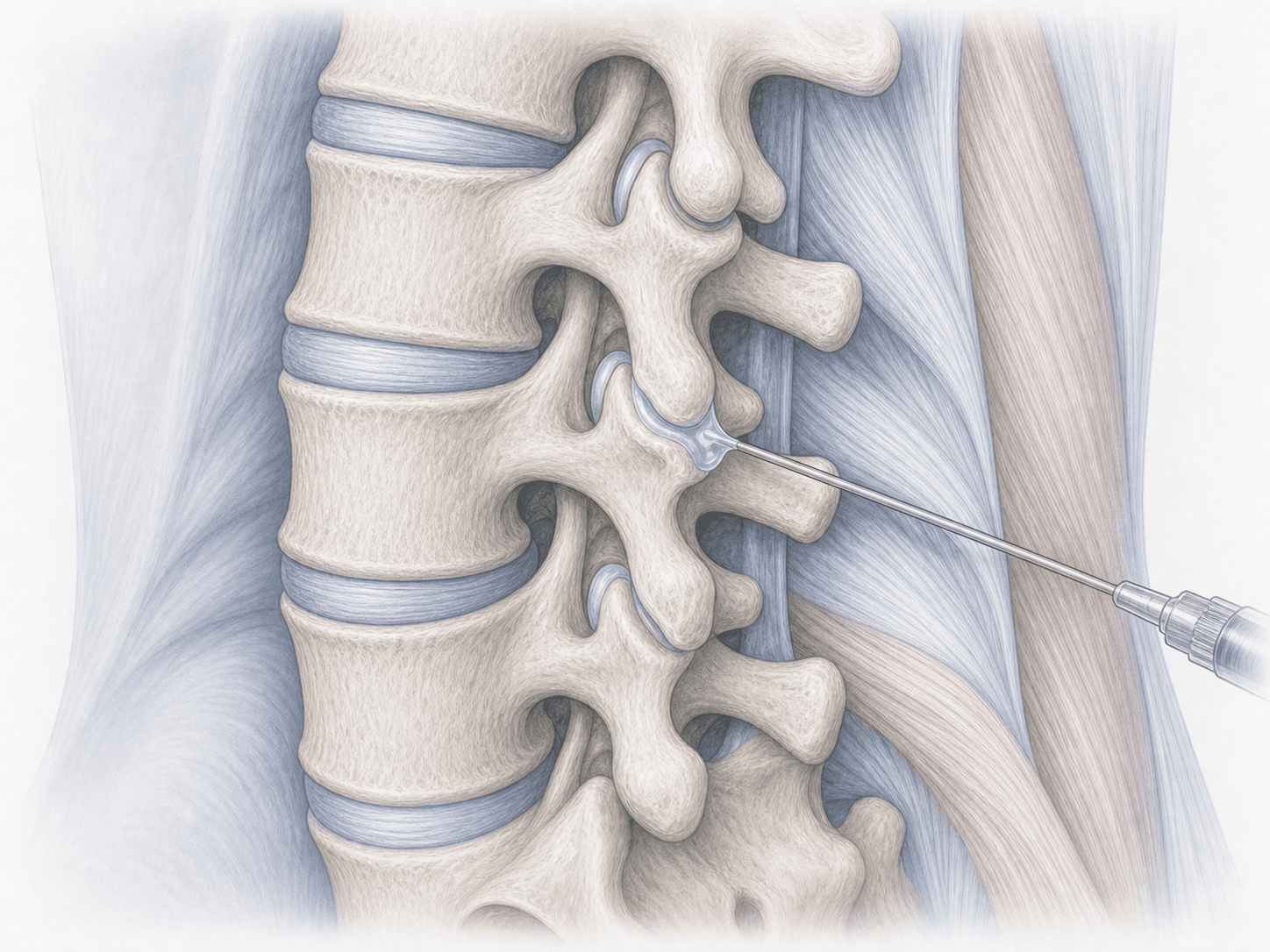
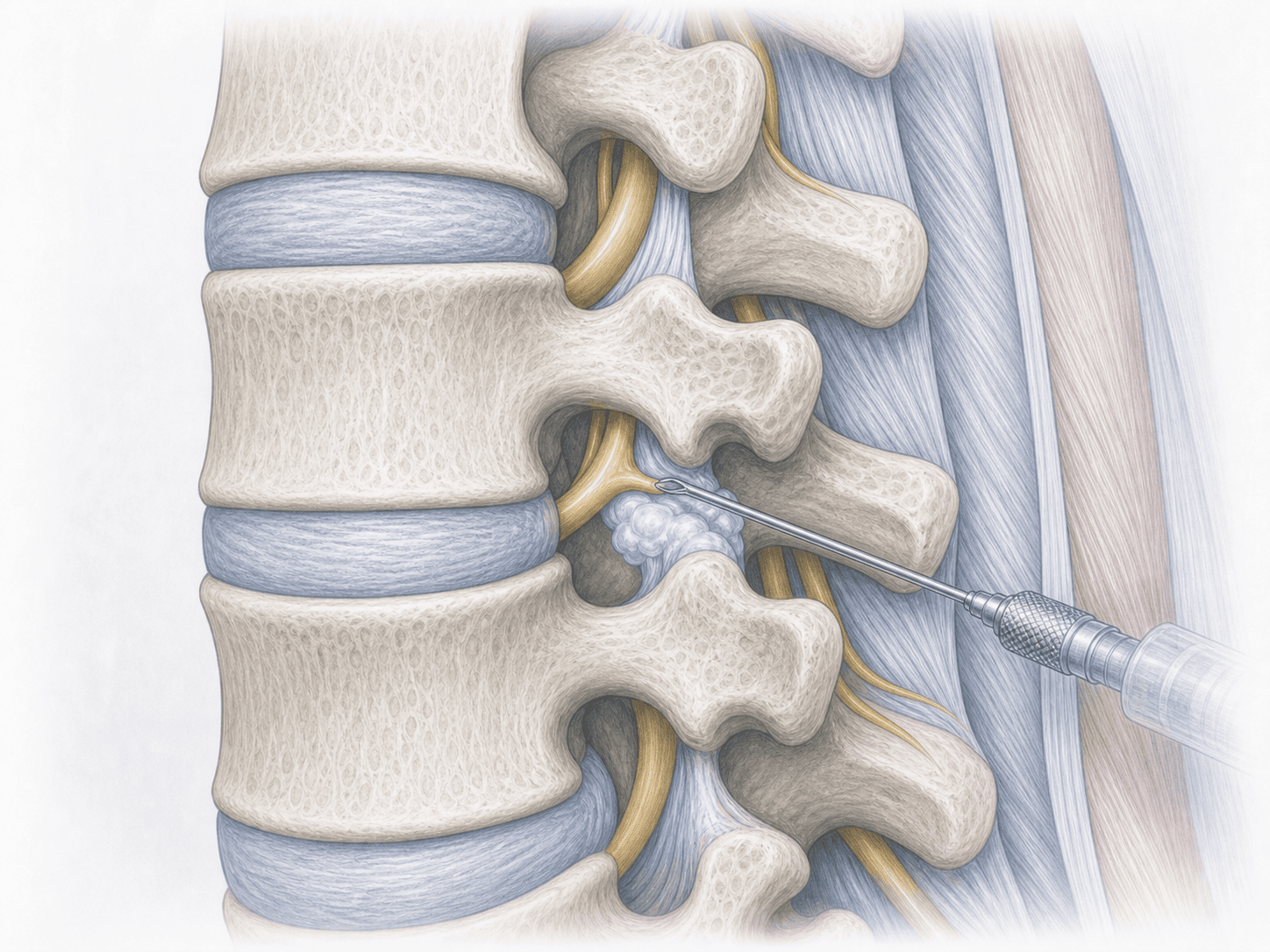
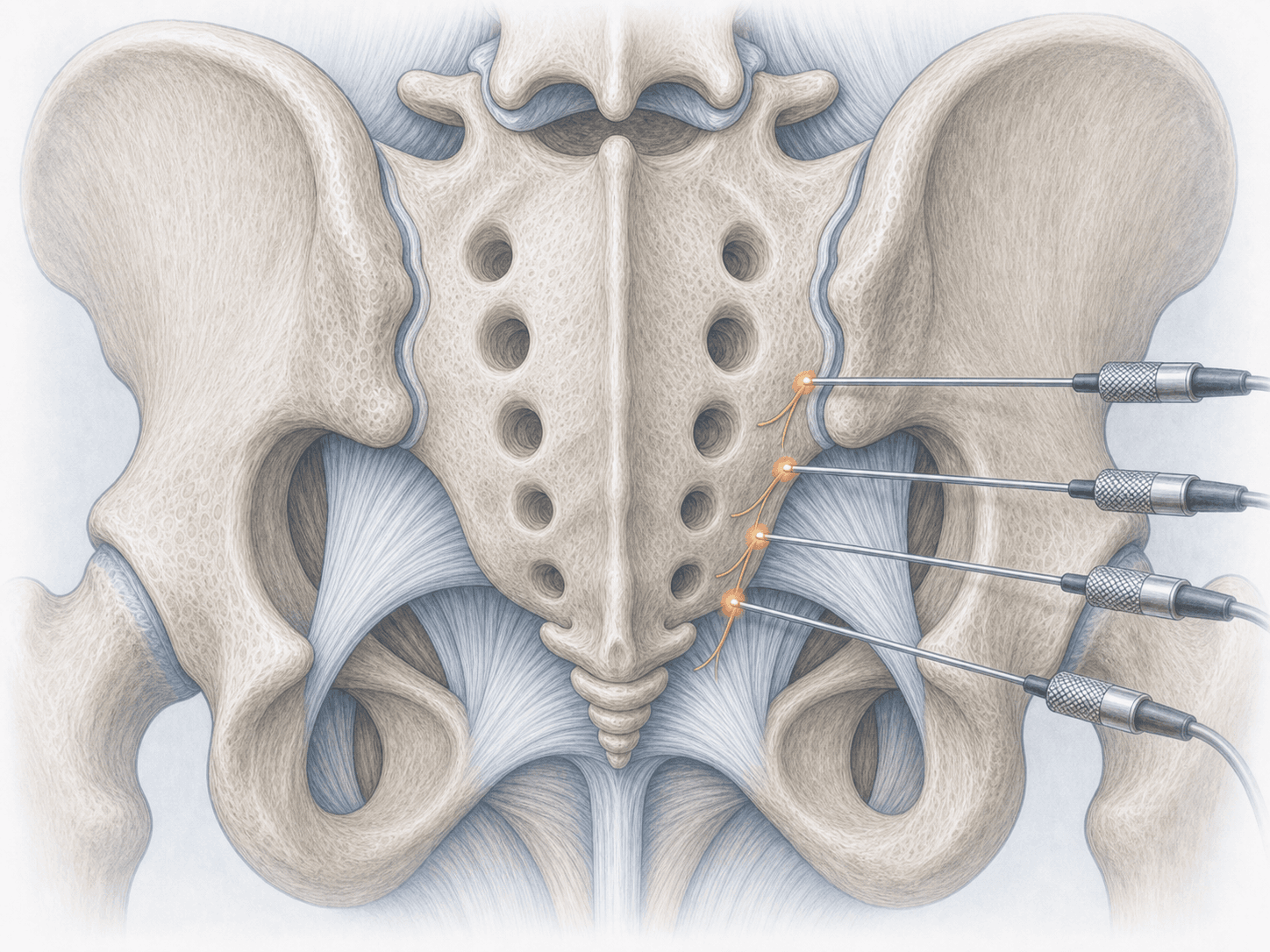
Unlike epidural injections, which target radicular pain from a herniation or stenosis, the sacroiliac block specifically addresses the joint between the sacrum and the ilium. If relief is clear but short-lived, the usual next step is sacroiliac radiofrequency rhizolysis to extend the effect. To discuss your case you can request an assessment with Dr. Ben Ghezala.
Symptoms and signs pointing to a sacroiliac origin
The typical clinical picture of sacroiliac pain has fairly recognisable features:
When is a sacroiliac block indicated?
How is the block performed step by step?
1.Preparation before the block
Before the procedure your MRI and clinical examination are reviewed, the affected side is confirmed and contraindications such as active infection, contrast allergy or uncontrolled anticoagulation are ruled out. Strict fasting is rarely required, although a light meal is advised. You should arrive in comfortable clothing and, if possible, with someone to accompany you home.
2.During the block
The patient lies prone. After skin disinfection and local anaesthesia, the lower third of the sacroiliac joint is reached with a fine needle under real-time fluoroscopic or ultrasound guidance. A small amount of contrast confirms intra-articular position and then the mix of local anaesthetic and corticosteroid is injected. The procedure takes 15 to 25 minutes, is performed as an outpatient and rarely requires deep sedation.
3.After the block
You remain under observation for 30 to 60 minutes. Keeping a simple pain diary during the first 6 hours and the following days, noting the percentage of relief, is very useful. That record is the key information to decide the next step: if relief is clear but brief, radiofrequency rhizolysis is usually considered; if relief is sustained, the block can be repeated at intervals.
Recovery after a sacroiliac block
Recovery is quick and most patients go home the same day. During the first hours pain may improve markedly thanks to the anaesthetic; afterwards a 24–72 hour intermediate phase is common in which discomfort partially returns, before the corticosteroid reaches full effect between days 3 and 7.
Intense effort, impact sport and heavy lifting should be avoided for 48 hours, but walking and normal daily activity can resume the next day. If relief is good, this is the ideal moment to reinforce physiotherapy and lumbopelvic stability work. Fever, marked redness at the site, leg weakness or disproportionate pain require prompt medical contact.
Risks and possible complications
Sacroiliac blocks are safe when performed under image guidance, but, as with any injection, risks should be discussed before signing consent.
The most common are mild: transient pain or bruising at the puncture site and a flare-up of pain 24 to 72 hours afterwards. Less frequently, facial flushing from the corticosteroid, insomnia or a temporary rise in blood sugar in patients with diabetes may occur. Serious complications are rare: infection, allergic reaction to the contrast or steroid, nerve injury or significant bleeding. Pregnancy and active infection are contraindications.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala