Lumbar foraminotomy
Lumbar foraminotomy is a procedure aimed at relieving radicular leg pain (sciatica or cruralgia) caused by compression of a nerve root within the intervertebral foramen. Many patients reach the clinic after months of low back and leg pain that has not improved with physiotherapy, injections or medication, and they fear a fusion that could limit their mobility. Foraminotomy decompresses the nerve root while preserving the facet joint and, in most cases, without fusing the segment. In this guide we explain when it is indicated, how we perform it and what to expect during recovery, so you can decide calmly and with honest information.
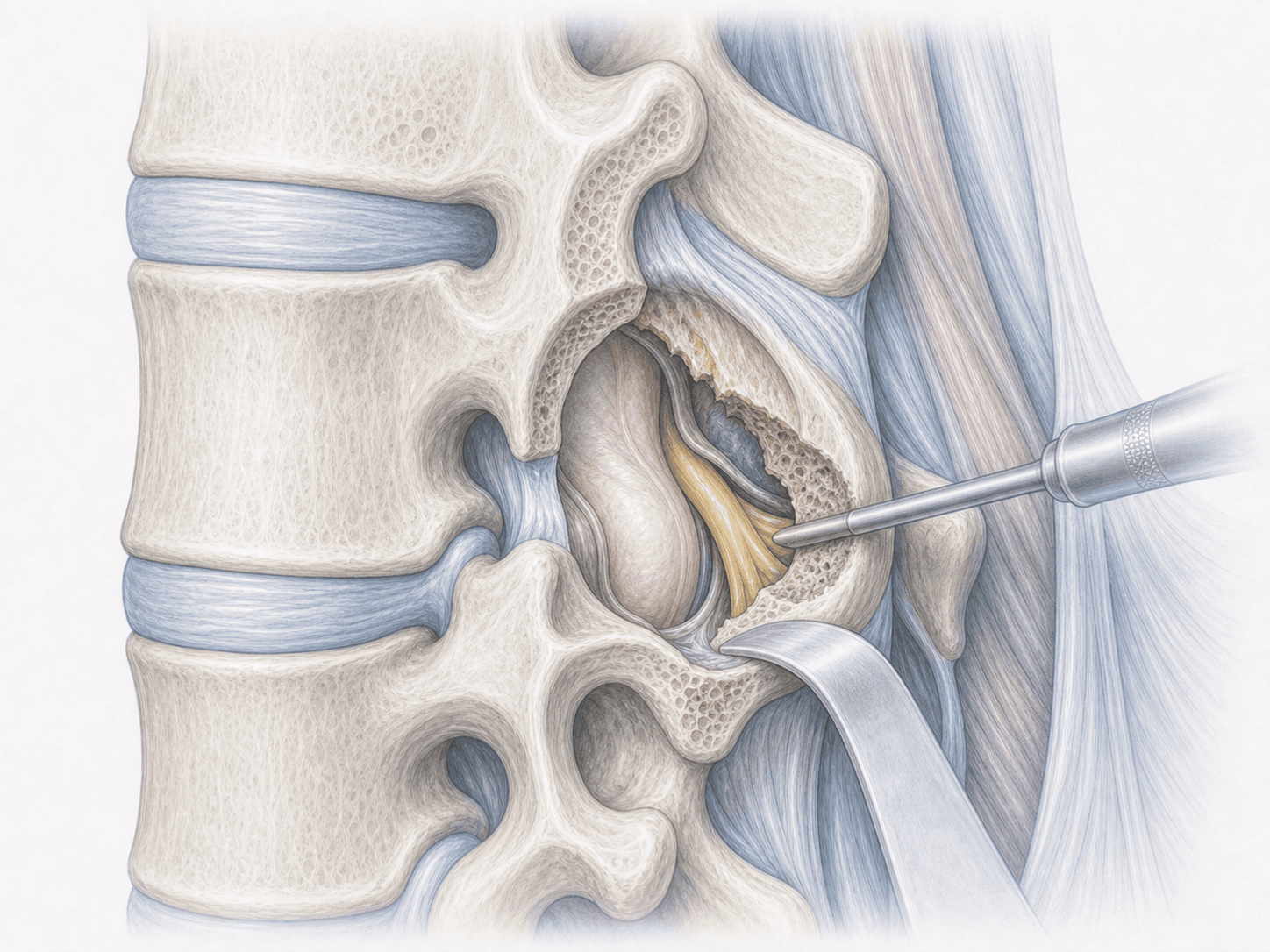
What is lumbar foraminotomy?
Lumbar foraminotomy is a microsurgical procedure that widens the intervertebral foramen —the opening through which the nerve root exits the spinal canal toward the leg— to free a root compressed by a foraminal disc herniation, osteophytes or stenosis. We perform it under the microscope and, whenever possible, with a minimally invasive approach, preserving most of the facet joint to maintain segmental stability.
Unlike cervical foraminotomy, here we work on the lumbar spine and the main goal is to relieve radicular leg pain without fusing the level. If you wish to discuss your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from a lumbar foraminotomy typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
We review your MRI together and, when needed, dynamic X-rays to rule out instability. We address your questions, adjust your usual medication (anticoagulants, anti-inflammatories) and give fasting instructions. If weight, smoking or other factors may influence recovery, we discuss them before surgery.
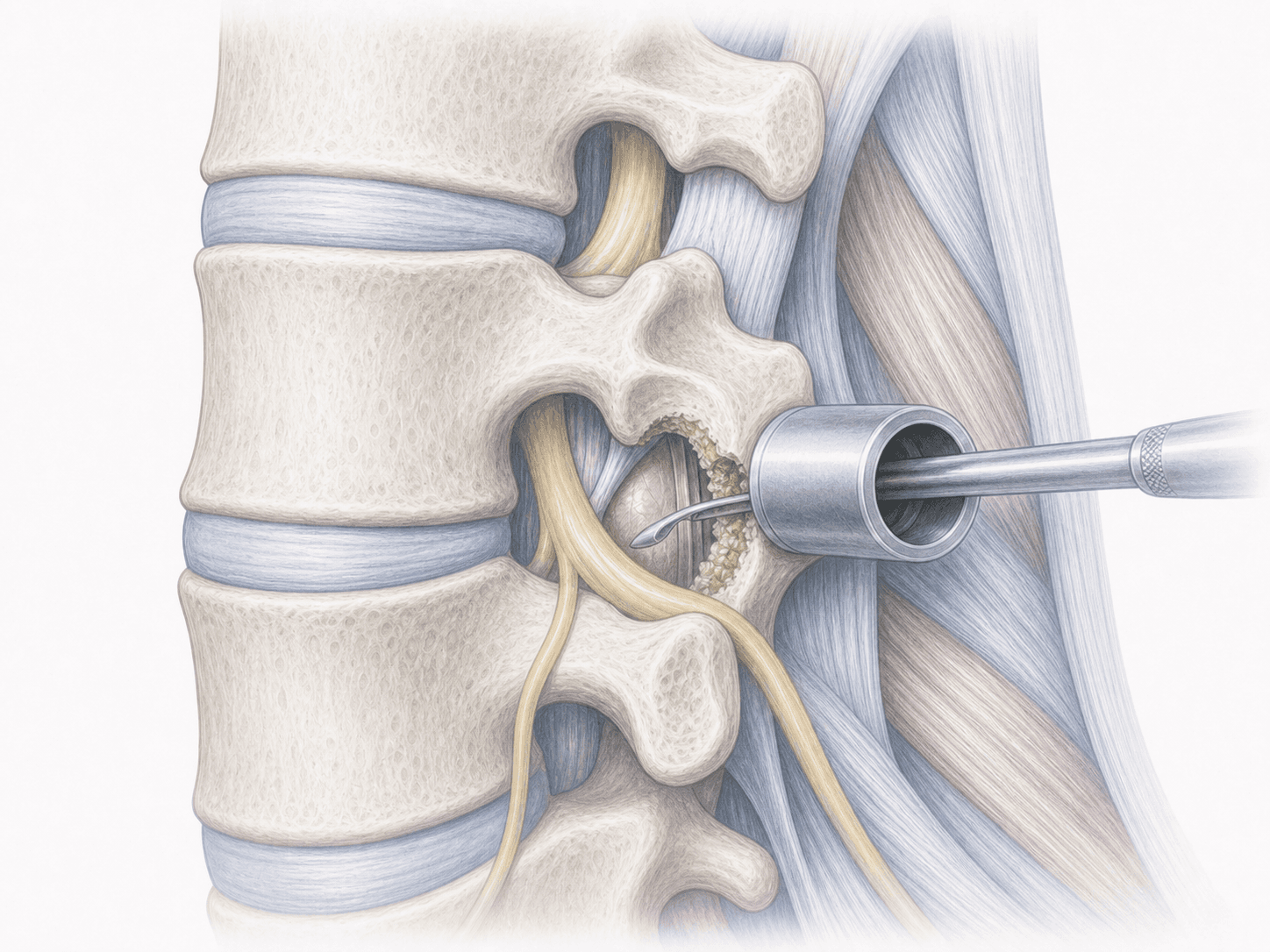
2.During the procedure
Under general anaesthesia, we use a small posterior approach centred on the affected level. With the microscope (and in selected cases an endoscopic technique), we identify the foramen, remove the osteophytes and disc material compressing the nerve root, and carefully widen the foraminal canal while preserving most of the facet joint. We confirm that the root is free and mobile before a layered closure.
3.Immediate postoperative period
After surgery you spend a short time in recovery before returning to your room. Most patients stand up the same day or the following morning with assistance. Hospital stay is typically around 24 hours, with tailored pain control.
Recovery after lumbar foraminotomy
Recovery is usually quick because we preserve most of the bony structures. Radicular leg pain often improves within the first days, while low back discomfort and residual numbness may take several weeks to fade.
Daily activities are typically resumed within the first week. Office work is usually possible after 2–4 weeks, and physically demanding jobs after 6–8 weeks. We recommend daily walking from the start, avoiding heavy lifting initially and starting guided physiotherapy when we indicate. Fever, sudden worsening of pain or new neurological deficits warrant prompt medical review.
Risks and possible complications
General surgical risks include infection, bleeding, thrombosis or anaesthesia-related issues.
Specific risks of lumbar foraminotomy include nerve root injury, cerebrospinal fluid leak from a small dural opening, recurrence of pain from a new herniation or epidural scar tissue and, less frequently, segmental instability if more bone than expected needs to be removed. In such cases an additional procedure may be considered later. These risks are assessed individually before recommending surgery.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala