Thoracic kyphoplasty
Thoracic kyphoplasty is a minimally invasive technique we perform through a small incision in the back. We insert a balloon into the fractured vertebral body, inflate it to restore height and fill the cavity with bone cement. We consider it when a vertebral fracture from osteoporosis, tumour or trauma causes severe pain that does not improve with rest, brace or analgesia after a few weeks. This guide helps you understand when it is indicated, how we perform it, what to expect afterwards and which risks it carries, so you can make a calm, informed decision.
What is thoracic kyphoplasty?
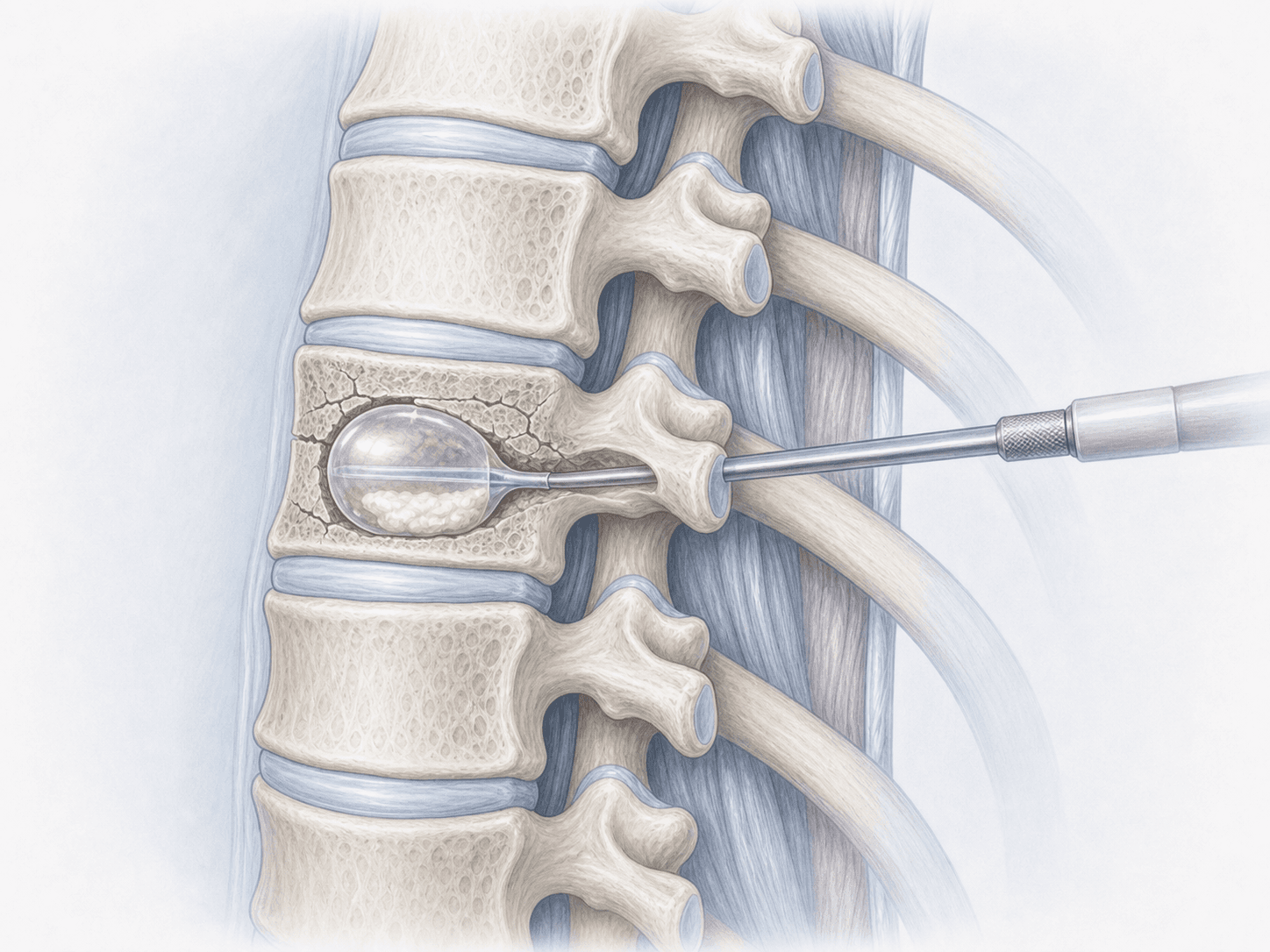
Thoracic kyphoplasty is a percutaneous technique to treat fractures of the vertebral body in the thoracic spine. Through a small incision we advance a trocar under fluoroscopic guidance into the vertebra. We then inflate a balloon to create a cavity and recover lost height, and finally fill that cavity with polymethyl methacrylate (PMMA) bone cement.
Unlike thoracic vertebroplasty, which injects cement directly without a balloon, kyphoplasty adds the step of creating a controlled cavity. This helps restore part of the vertebral body height and reduces the risk of cement leakage. To discuss your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from thoracic kyphoplasty typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
We review the MRI to confirm an active fracture and the X-ray or CT to plan the trocar trajectory. We provide fasting instructions, adjust anticoagulant medication if needed and answer your questions calmly. If a tumour-related fracture is suspected, we consider a biopsy during the same procedure.
2.During the procedure
You are placed face down under local anaesthesia with sedation or, depending on the case, general anaesthesia. Through a small incision we introduce a trocar into the vertebral body under fluoroscopic guidance. We inflate the balloon to create a cavity and recover part of the height, remove the balloon and fill the cavity with high-viscosity PMMA cement. The procedure usually lasts 30 to 60 minutes per vertebra.
3.Immediate postoperative period
You rest in bed for about two hours while the cement fully sets. We then check that you can stand up and walk safely. Many patients notice pain relief within the first few hours. Discharge is usually the same day or after one night of observation, depending on your overall condition.
Recovery after thoracic kyphoplasty
Functional recovery is usually quick. Most patients resume daily activities within a few days, with gentle walking from the start. We recommend avoiding lifting weights or sudden efforts for 4 to 6 weeks to protect the treated and adjacent vertebrae.
The acute fracture pain typically improves noticeably within the first 24 to 72 hours. Background treatment of osteoporosis or the underlying tumour remains essential to reduce the risk of new fractures. New fever, chest pain, breathing difficulty or any neurological deficit warrants prompt medical review.
Risks and possible complications
Any procedure carries general risks such as infection, bleeding, anaesthesia-related issues or thrombosis.
Specific risks of thoracic kyphoplasty include cement extravasation into the epidural space, disc or veins (most are asymptomatic), pulmonary cement embolism (uncommon), rib fracture or adjacent vertebral fracture and, exceptionally, neurological injury. We assess each case individually to minimise these risks.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala