Posterior thoracic fusion
Posterior thoracic fusion is surgery that stabilises the dorsal spine from the back using pedicle screws and rods. It is considered when a fracture, deformity, tumour or instability threatens the spinal cord or seriously limits daily life. Many patients reach this option after trauma, an osteoporotic compression fracture or progressive pain that does not respond to conservative care. Others present with adult scoliosis, spondylitis or tumour lesions that need posterior reinforcement. This guide explains when it is indicated, how it is performed and what to expect during recovery, so that you can make a calm, informed decision with a team experienced in spine surgery.
What is posterior thoracic fusion?
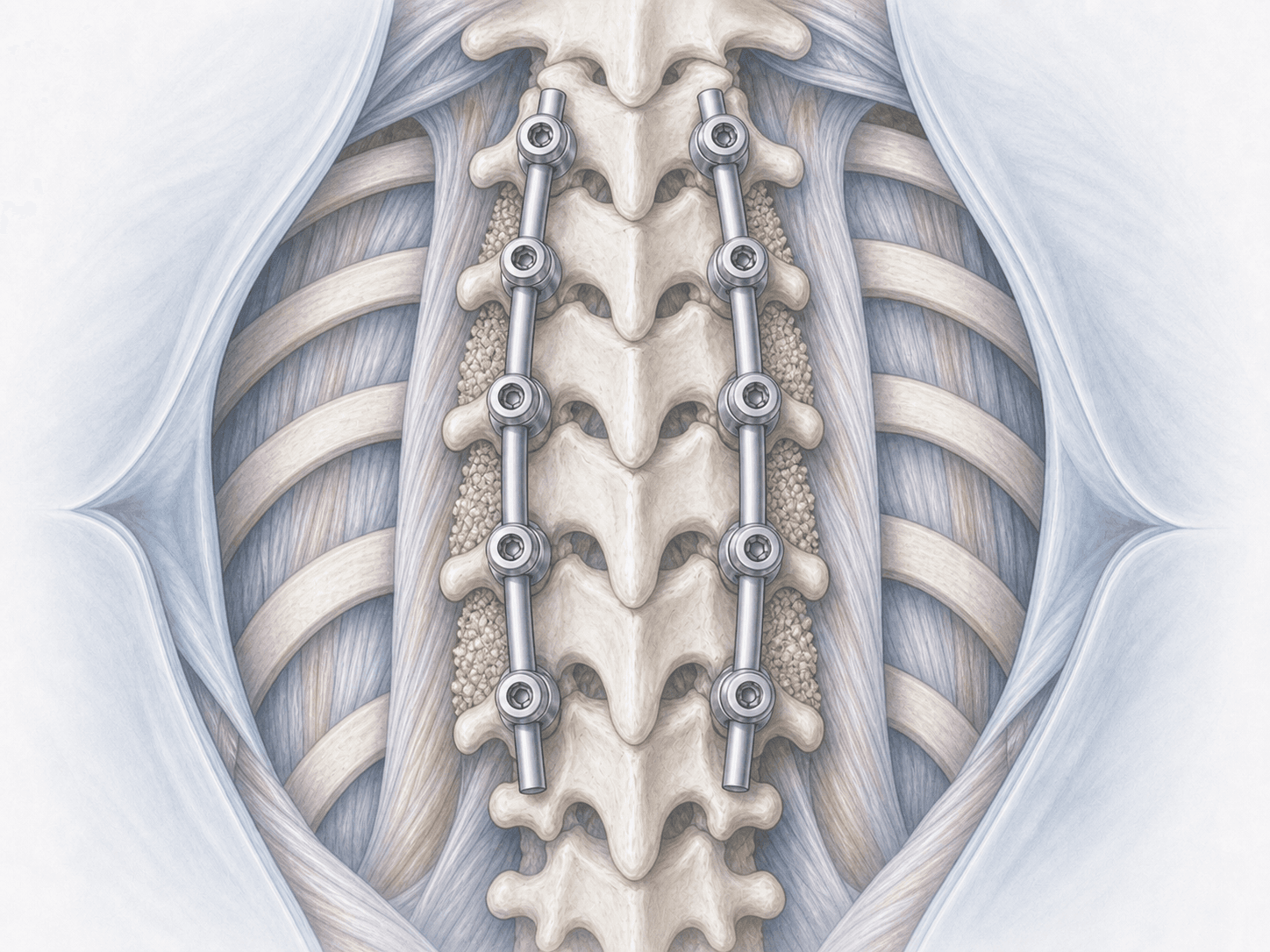
Posterior thoracic fusion is a surgery that stably joins one or several levels of the dorsal spine (T1 to T12) through a posterior approach. We place pedicle screws in the vertebral bodies and connect them with metal rods. Bone graft is then added so the segment can fuse over time.
Unlike cervicothoracic fusion, which focuses on the junction between the lower cervical and upper thoracic spine, this technique addresses the pure thoracic spine. The proximity of the spinal cord, pleura and great vessels demands careful planning and, when needed, intraoperative navigation and neuromonitoring. If you want to discuss your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from posterior thoracic fusion typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
We carry out a full clinical assessment, review the MRI and CT, assess bone density when osteoporosis is suspected and plan the levels to be instrumented. Fasting rules, anticoagulant adjustments and antibiotic prophylaxis are tailored to thoracic surgery in our centres in Alicante and Benidorm.
2.During the procedure
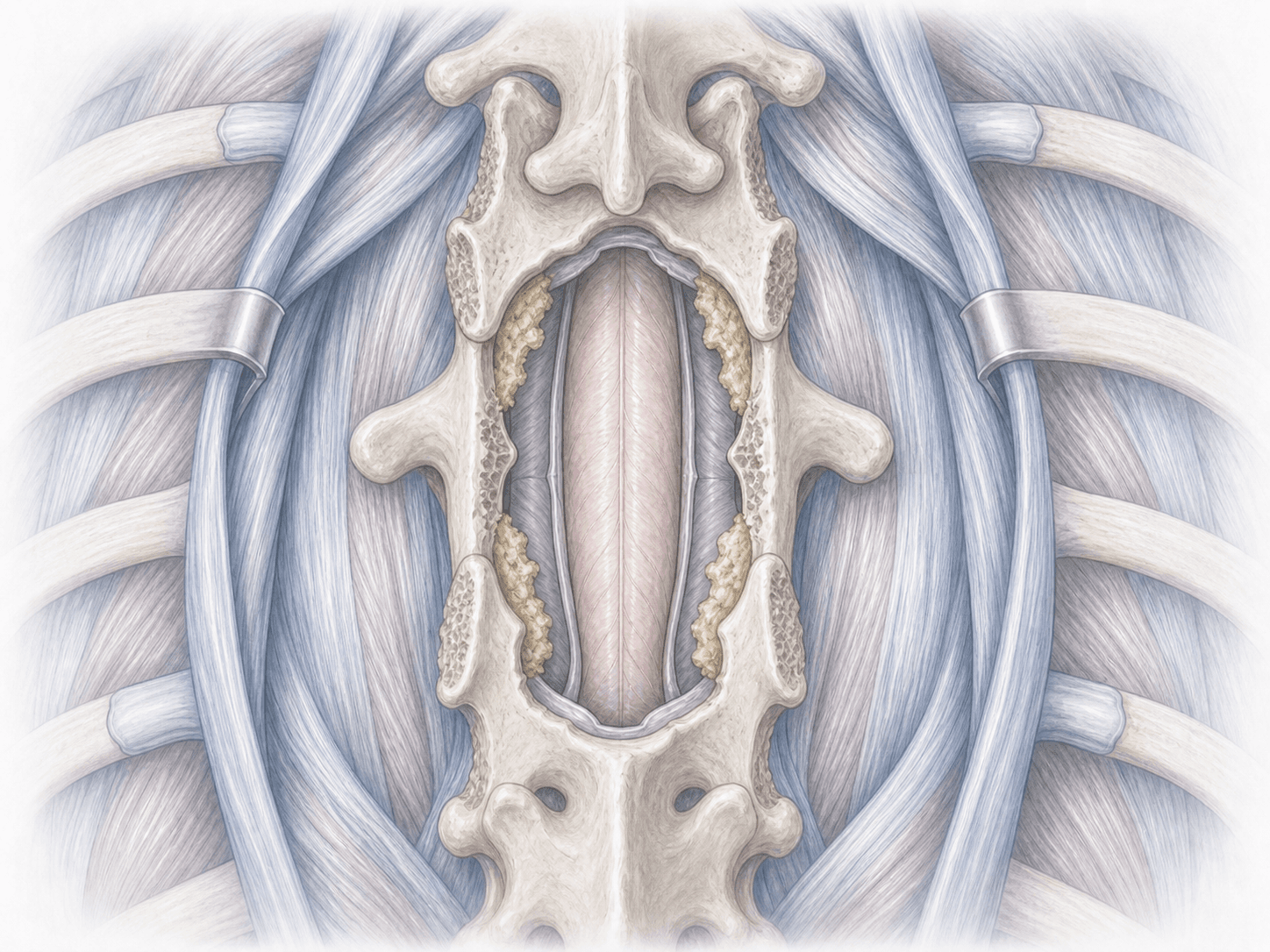
The patient is placed prone under general anaesthesia. We use a posterior approach centred on the levels to be treated. Pedicle screws are inserted in each vertebra under fluoroscopy and, when the case calls for it, neuronavigation, given the proximity of the pleura, aorta and spinal cord.
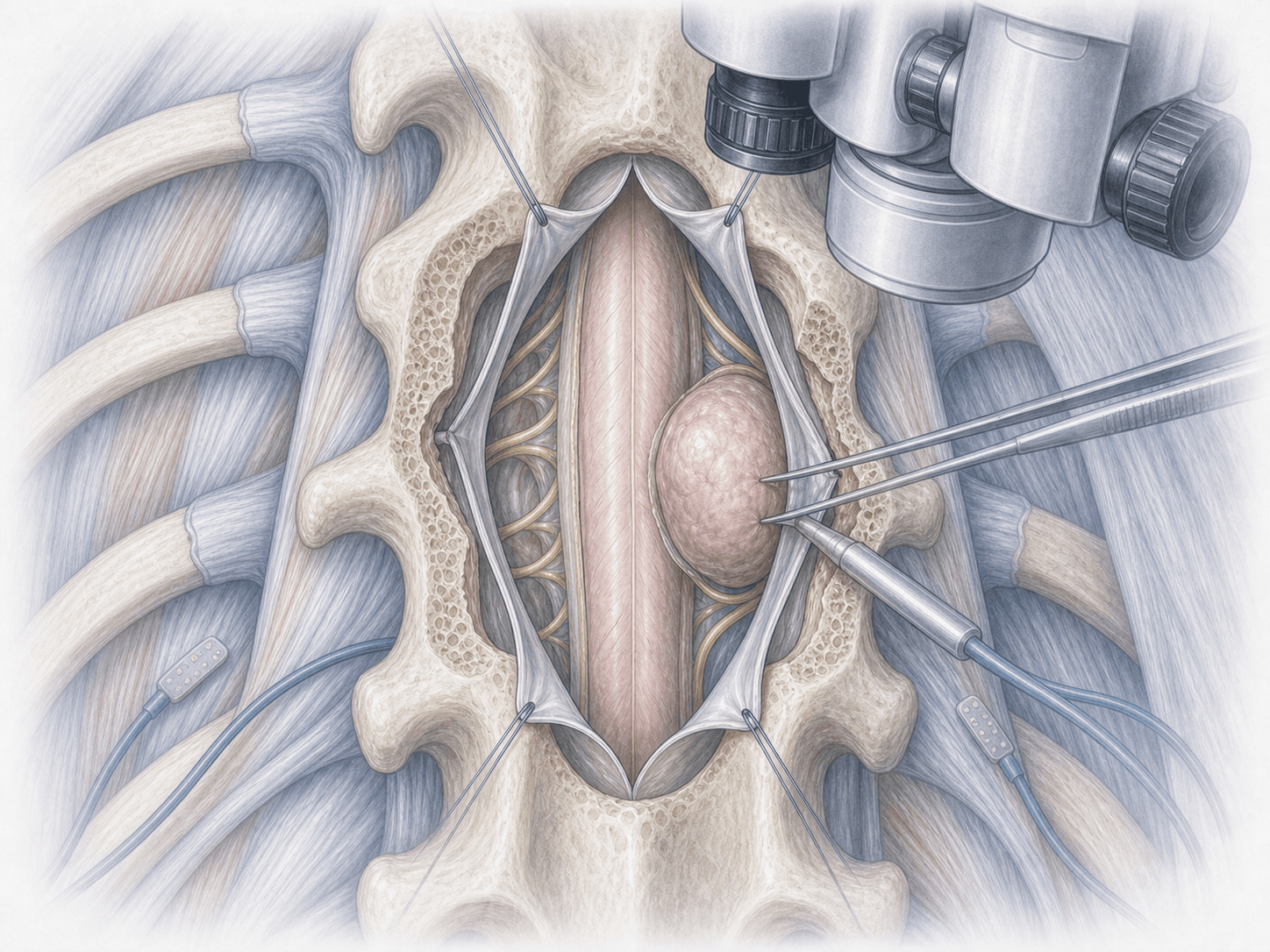
Intraoperative neurophysiological monitoring tracks the cord and nerve roots throughout. When needed, we decompress the spinal cord by removing lamina or compressing bone. The screws are then connected with two rods, the deformity is corrected if appropriate and bone graft is added to promote fusion.
3.Immediate postoperative period
Patients spend several hours in recovery and, in many cases, one night under close neurological observation. We start multimodal analgesia and progressive mobilisation the following day, supported by physiotherapy. Hospital stay typically ranges from 3 to 7 days depending on the number of fused levels and the underlying cause.
Recovery after posterior thoracic fusion
Recovery is gradual. Assisted walking usually starts the day after surgery and light activities resume within a few weeks. Office work is typically possible between 6 and 12 weeks. Physical jobs need longer and are always assessed case by case.
Bony fusion takes several months to consolidate, so heavy axial loads, abrupt twisting and impact sports are avoided early on. Specific rehabilitation, postural hygiene and scheduled imaging follow-up shape the outcome. Fever, worsening pain or new neurological symptoms warrant prompt review.
Risks and possible complications
Every surgery carries general risks such as infection, bleeding, thrombosis or anaesthesia-related complications.
Specific risks of posterior thoracic fusion include misplacement of a pedicle screw, with possible nerve root irritation or injury to the spinal cord, vessels or pleura. Cerebrospinal fluid leak, pneumothorax (uncommon), non-union (pseudarthrosis), loosening of the hardware or accelerated degeneration of adjacent levels may also occur. Individual planning, fluoroscopy, navigation when appropriate and neurophysiological monitoring help reduce these risks.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala