Intraspinal tumour surgery
Intraspinal tumour surgery is used to treat lesions growing inside the spinal canal, either outside the spinal cord (intradural extramedullary tumours such as meningiomas, schwannomas or neurofibromas) or within it (intramedullary tumours such as ependymomas, astrocytomas or haemangioblastomas). Receiving a diagnosis of a spinal tumour is understandably unsettling. Most of these lesions are benign and, when treated in time with appropriate microsurgical technique, can be removed with good functional outcomes. This guide explains realistically how surgery is planned, what to expect during recovery and which factors influence prognosis, so you can make an informed decision with calm.
What is intraspinal tumour surgery?
Intraspinal tumour surgery is a microsurgical procedure aimed at resecting tumours that develop inside the spinal canal at any level (cervical, thoracic, lumbar or sacral). Two main groups are distinguished: intradural extramedullary tumours, which grow around the spinal cord and are usually benign (meningiomas, schwannomas, neurofibromas); and intramedullary tumours, which arise within the spinal cord itself (ependymomas, astrocytomas, haemangioblastomas).
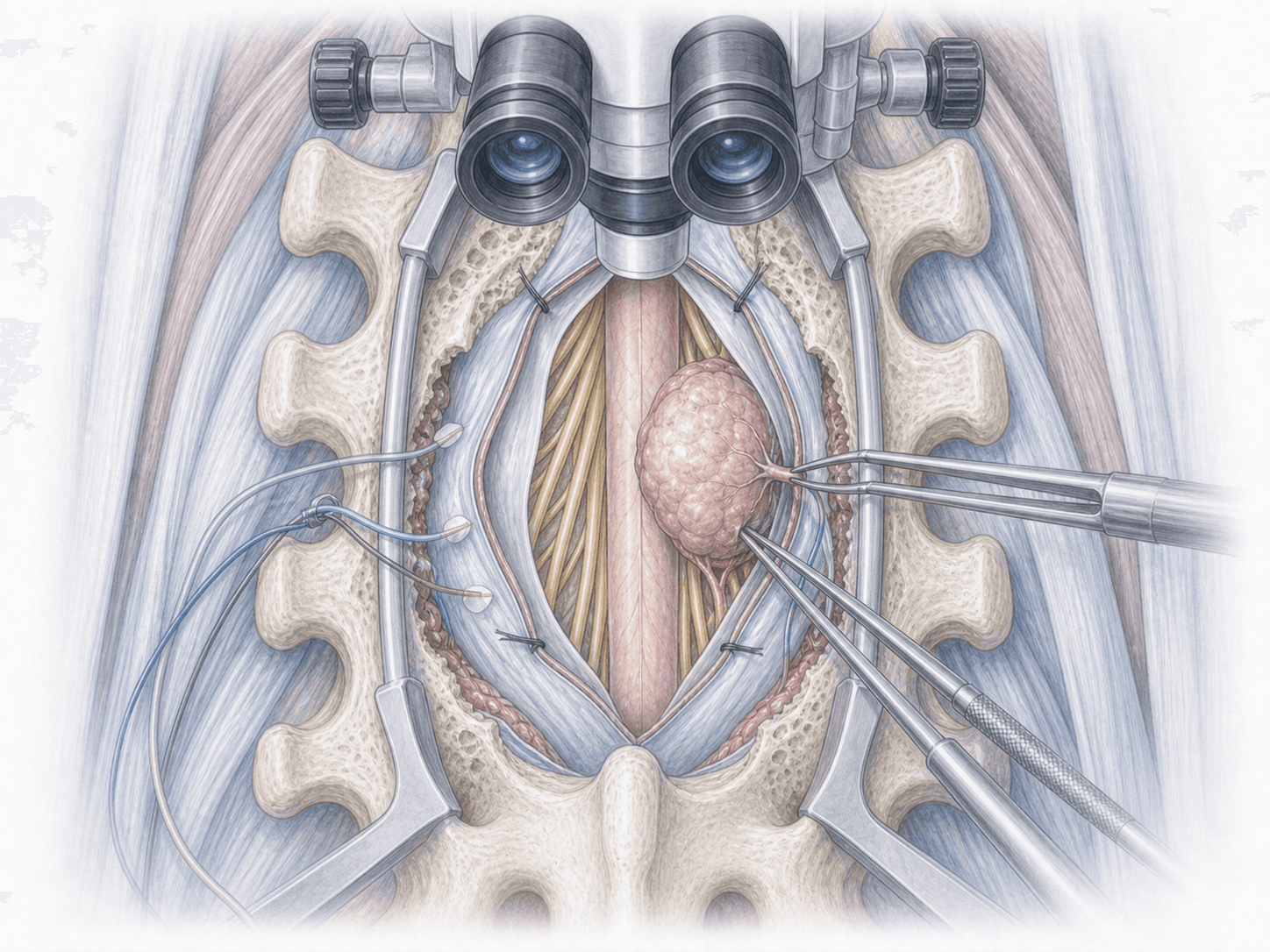
The goal is to achieve the most complete resection possible while preserving the functional integrity of the spinal cord and nerve roots. Surgery is performed under the operating microscope and with mandatory intraoperative neuromonitoring (motor and somatosensory evoked potentials), which allows continuous monitoring of neurological function throughout the procedure.
Unlike primary vertebral tumours, which affect the bone, intraspinal tumours sit inside the dural sac and require a specific technique of opening, resection and watertight closure. If you have received this type of diagnosis, you can request an assessment with Dr. Ben Ghezala to review your case in detail.
Symptoms and warning signs
Intraspinal tumours usually grow slowly, so symptoms tend to appear gradually and may initially be confused with other spinal problems. The most frequent manifestations are:
When is this surgery indicated?
How is the procedure performed?
1.Preoperative preparation
Includes a thorough clinical assessment, review of the contrast-enhanced MRI and, depending on the case, additional studies such as CT, angiography or baseline neurophysiological tests. The procedure is explained in detail, questions are addressed and the surgical strategy is planned together with the neuromonitoring team. Fasting instructions, medication adjustments (particularly anticoagulants) and recommendations tailored to the affected level are provided.
2.During the procedure
Under general anaesthesia and with continuous intraoperative neuromonitoring, the spinal canal is accessed through a laminotomy or laminectomy at the level of the tumour. The dura is carefully opened and, under the operating microscope, the lesion is identified.
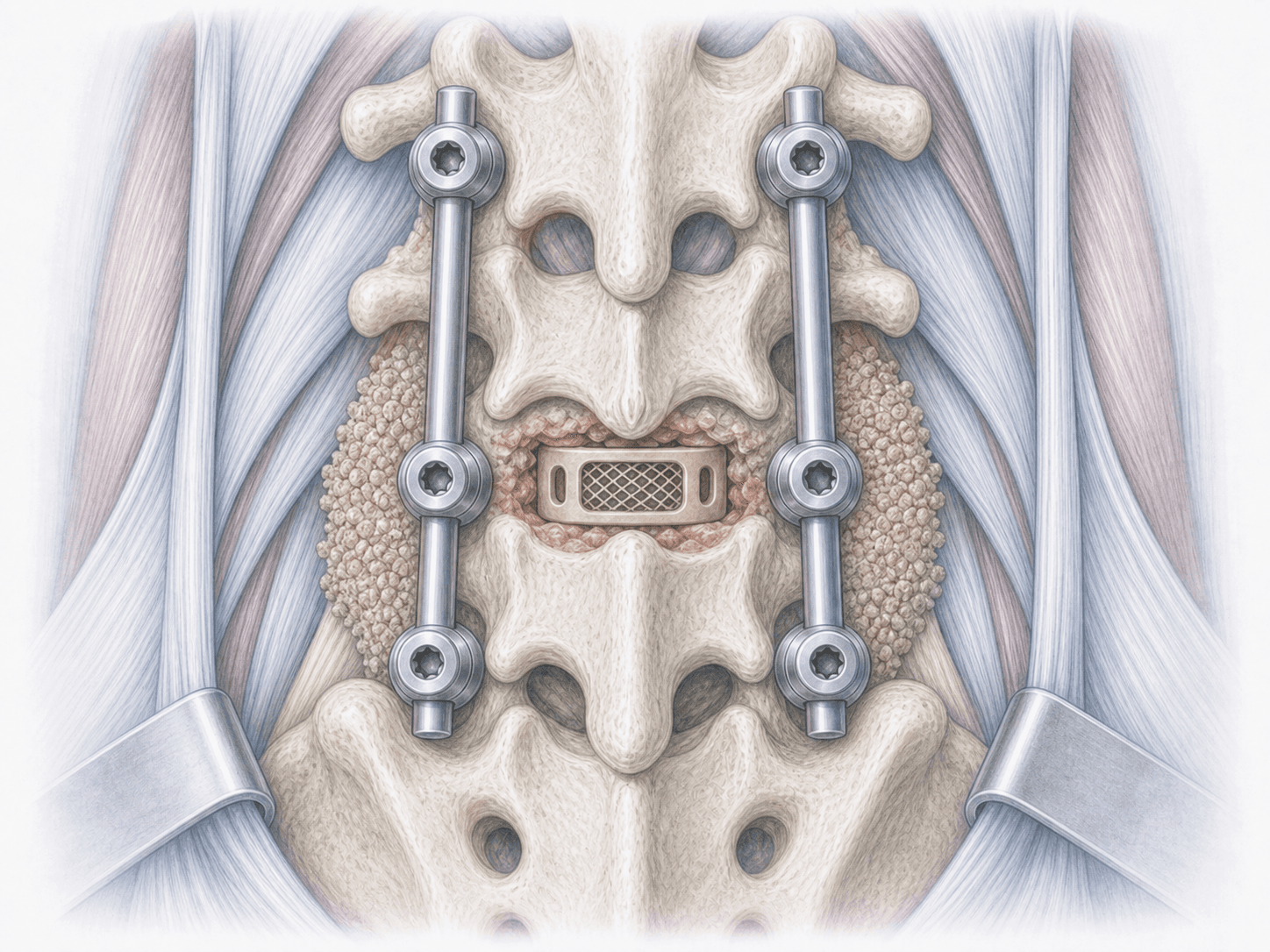
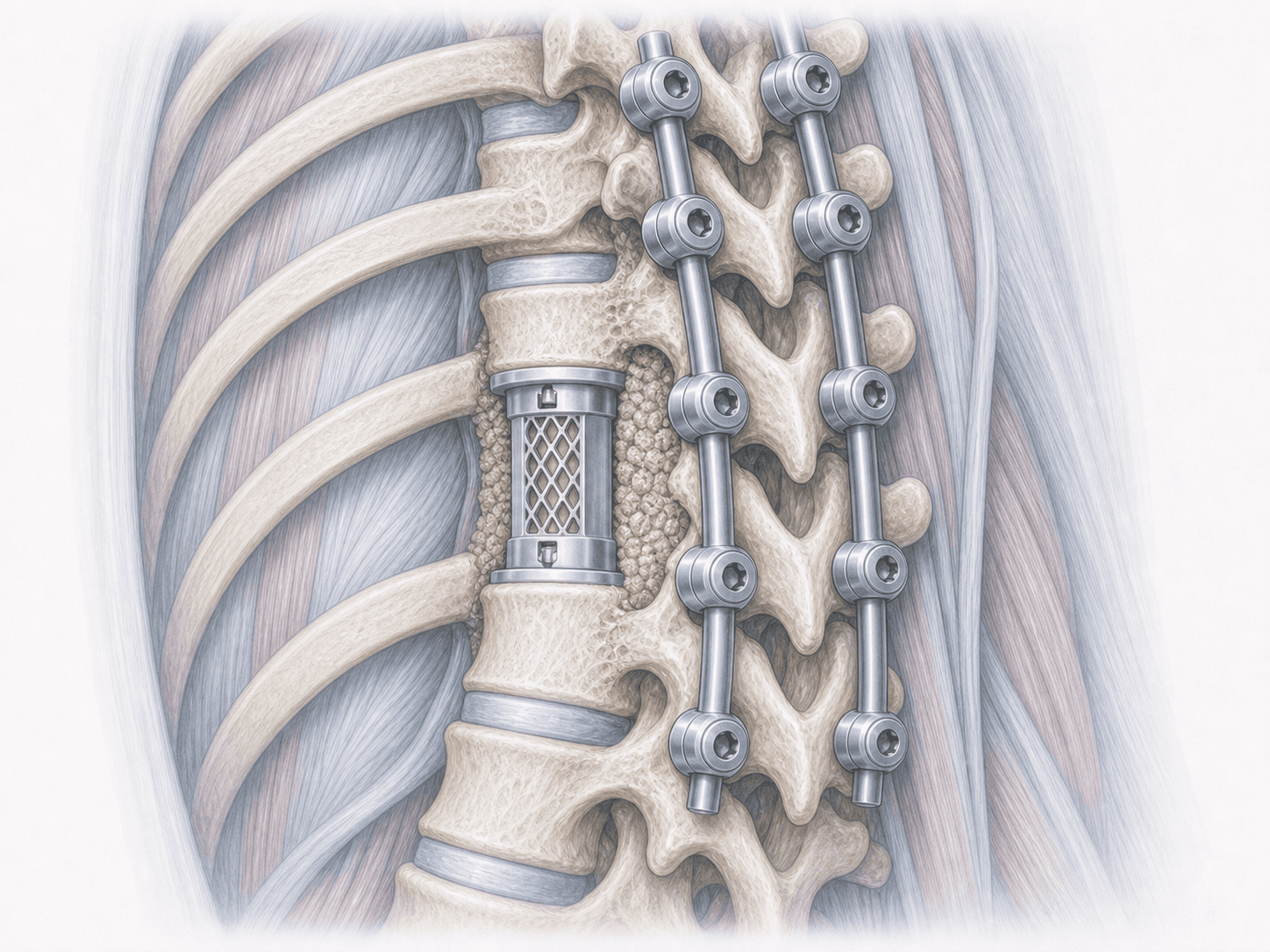
In intradural extramedullary tumours (meningiomas, schwannomas) resection is usually complete and respects the spinal cord. In intramedullary tumours a midline myelotomy is performed to reach the tumour and resect as much tumour tissue as is compatible with preservation of function, guided by neuromonitoring. A watertight dural closure is performed at the end and, if stability is compromised, complementary instrumentation is considered.
3.Immediate postoperative period
Patients spend the first hours in a monitored unit where neurological function, pain and the surgical wound are observed. Progressive mobilisation is started according to the level operated and patient tolerance. Hospital stay is typically 4 to 7 days for intradural extramedullary tumours and may be longer for intramedullary tumours, depending on clinical progress and the need for early physiotherapy.
Recovery after intraspinal tumour surgery
Recovery depends on the type of tumour, its location and the preoperative neurological status. In completely resected benign intradural extramedullary tumours, pain relief is usually rapid and pre-existing neurological deficits often improve gradually over weeks or months.
In intramedullary tumours recovery is slower and neurological rehabilitation with physiotherapy plays a central role. Sensory deficits or some instability are common in the first weeks and tend to improve progressively with rehabilitation.
Follow-up includes clinical reviews and serial MRI scans to confirm the extent of resection and monitor for recurrence, especially in lesions with more complex histology. Fever, wound leakage, severe pain or new neurological deficits require immediate medical contact.
Risks and possible complications
Every surgery carries general risks such as infection, bleeding, thrombosis or anaesthesia-related complications.
Specific risks of intraspinal tumour surgery include transient or permanent neurological worsening (motor, sensory or sphincter deficit), cerebrospinal fluid leak, postoperative haematoma, deep infection, spinal instability after wide laminectomies (sometimes requiring instrumentation) and, in tumours with complex histology, the possibility of incomplete resection or recurrence. These risks are assessed and explained individually before deciding on surgery.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala