Microscope-assisted spinal surgery
Microscope-assisted spinal surgery is the modern standard in spine neurosurgery: it provides 6 to 20-fold magnification of every nerve, dural and vascular structure within the surgical field. Many common techniques —microdiscectomy, canal decompressions, intradural tumour surgery or dural fistula repair— rely on the microscope precisely because it offers the stable, illuminated and shared view that spinal surgery requires. This guide explains what changes for you as a patient when a procedure is performed with a surgical microscope, when it is especially useful and what to expect before, during and after.
What is microscope-assisted spinal surgery?
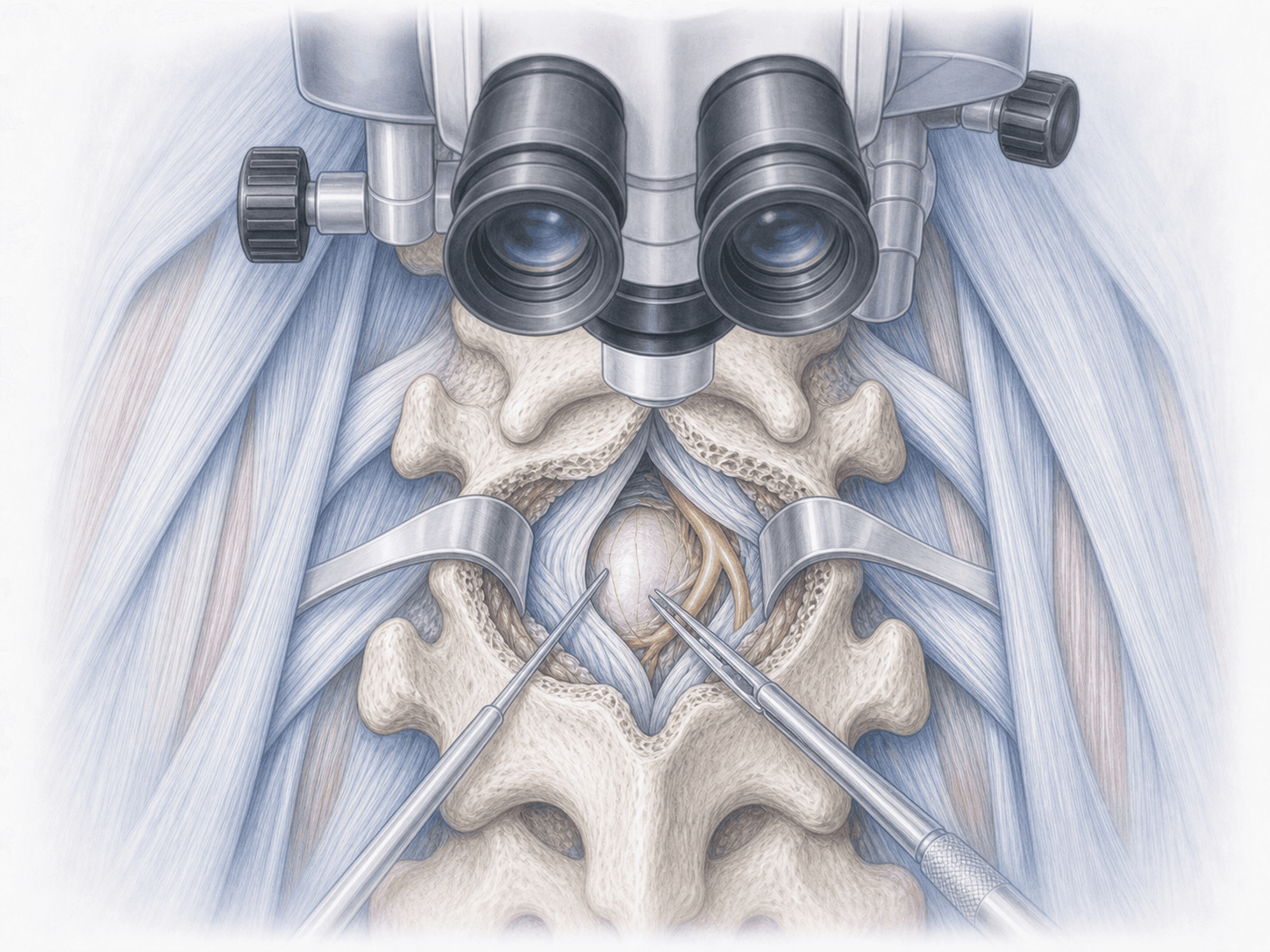
Microscope-assisted spinal surgery is the technique that uses a stereoscopic surgical microscope, with variable 6 to 20-fold magnification and coaxial illumination, to operate on the spine with the highest possible precision over delicate structures: nerve roots, spinal cord, dura mater and blood vessels.
Unlike surgical loupes, the microscope provides true binocular vision, depth of field, light aligned with the visual axis that reaches the bottom of the canal and the possibility for the entire surgical team to share the same view through integrated cameras. That is why it is the gold standard in procedures such as lumbar microdiscectomy, spinal cord decompressions and intradural tumour surgery. To assess whether your case may benefit from this technique, you can request an assessment with Dr. Ben Ghezala.
When is microscope-assisted surgery used?
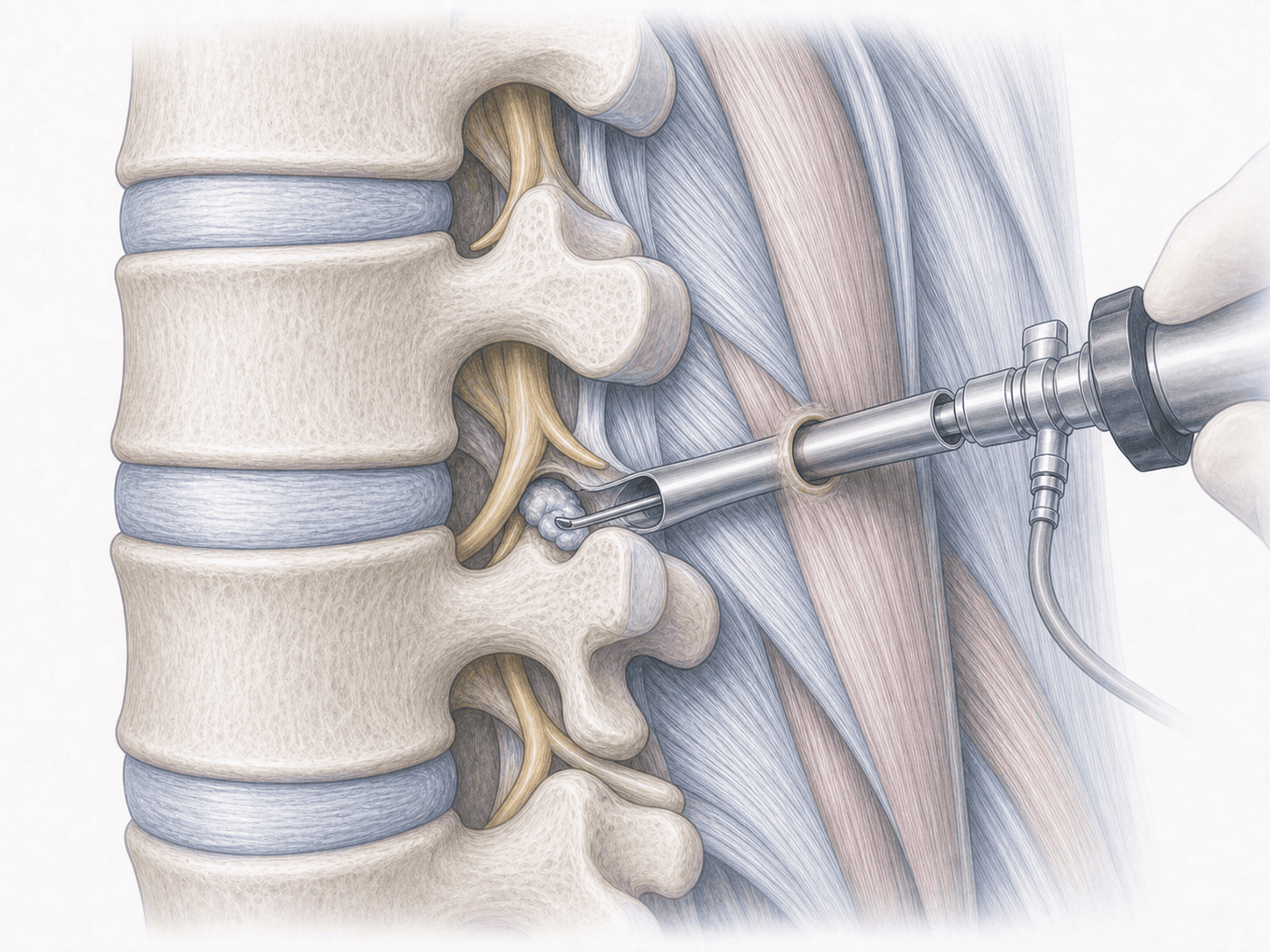
The surgical microscope is used in spinal procedures where magnified visualisation of neural structures makes a real difference. Typical situations include:
When is this technique indicated?
How is the procedure performed?
1.Preoperative preparation
Using the microscope does not change your preparation as a patient. Clinical assessment is performed, imaging is reviewed and the exact level to be treated is planned. Fasting instructions, medication adjustments and specific recommendations are provided depending on the particular procedure in which the microscope will be used.
2.During the procedure
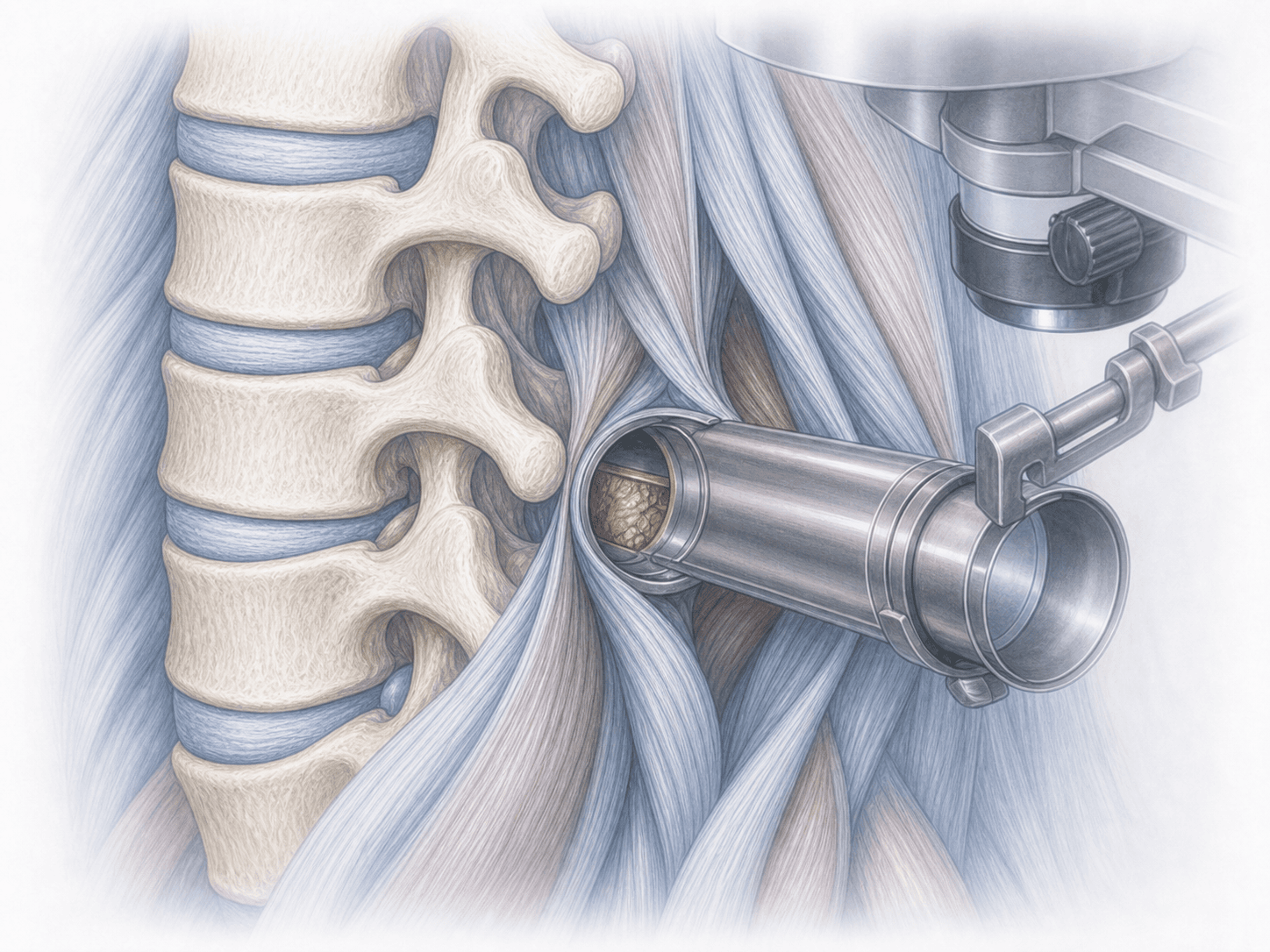
After the initial approach and bony opening, the surgical microscope is brought into the field. From that point onwards the entire surgery is performed looking through the microscope, with variable magnification and coaxial lighting. The surgeon adjusts focus, zoom and position without touching the sterile field through handgrip or foot controls. The team —assistant, scrub nurse and anaesthesia— follows the surgery on a screen connected to the microscope, improving coordination and safety.
3.Immediate postoperative period
The immediate postoperative period depends on the specific procedure, not on the use of the microscope itself. In general, pain is controlled, neurological status is monitored and early mobilisation begins. The reduced tissue trauma associated with microsurgery often translates into less postoperative pain and an earlier return to walking and basic daily activities.
Recovery after microscope-assisted surgery
Recovery depends mainly on the specific surgery: a lumbar microdiscectomy is very different from a cervical spinal cord decompression or the resection of an intradural tumour. The microsurgical technique, by reducing the size of the approach and preserving healthy tissue, tends to allow earlier mobilisation and lower painkiller use in the first days.
Return to work, driving, sport and physical activity is planned according to each procedure. As in any spinal surgery, fever, worsening pain, fluid leakage from the wound or new neurological symptoms warrant prompt medical review.
Risks and possible complications
The microscope itself does not add risks to the procedure; on the contrary, its purpose is to reduce neurological risk by allowing safer dissection. General and specific risks remain those of the underlying spinal surgery being performed: infection, bleeding, anaesthesia-related complications, thrombosis, neurological injury, dural tear with cerebrospinal fluid leak or recurrence of the treated problem.
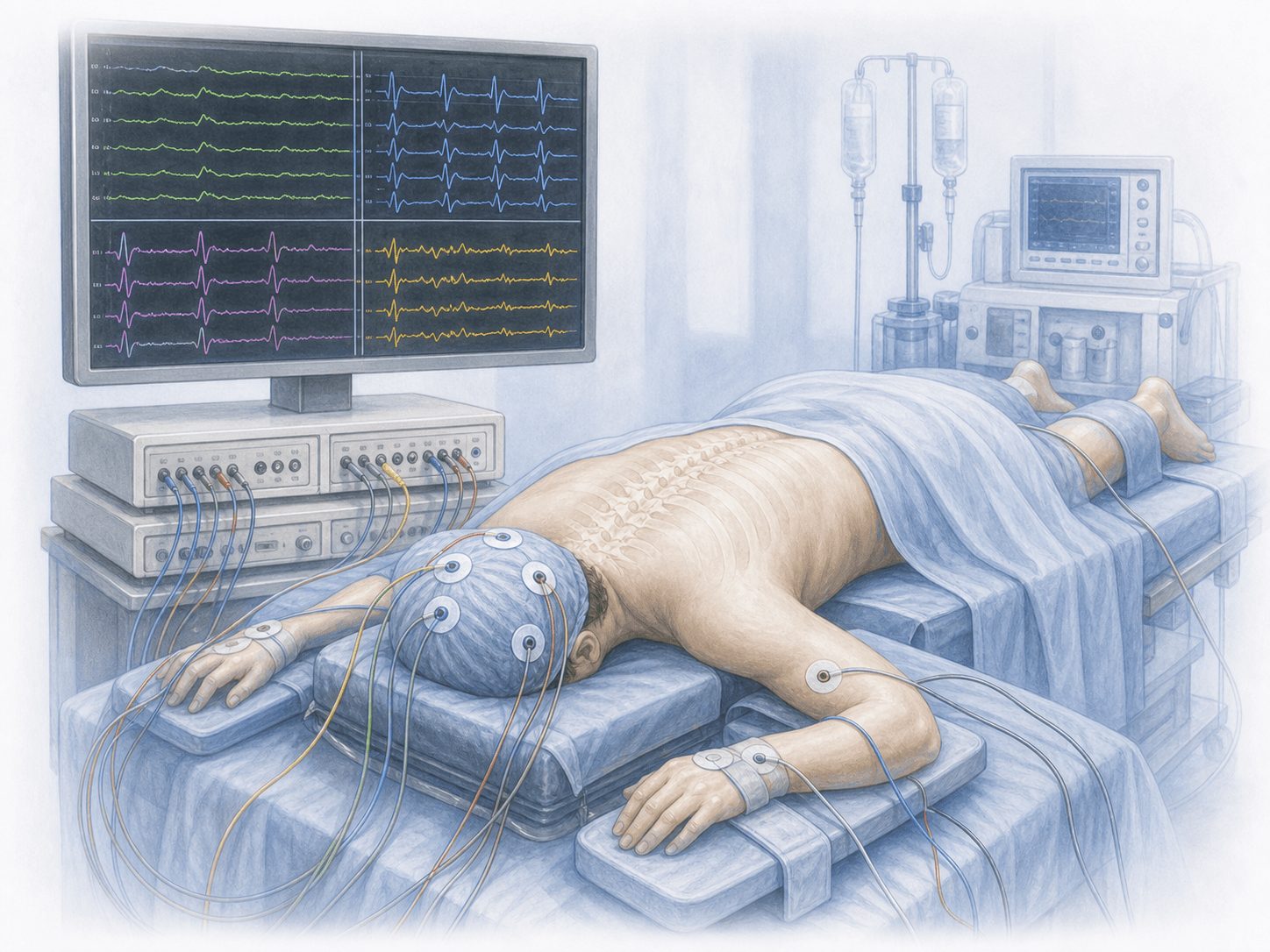
In complex cases the microscope is complemented with intraoperative neurophysiological monitoring and, when indicated, with neuronavigation. Each risk is assessed individually according to the specific procedure and the patient's condition.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala