Spine hardware removal
Spine hardware removal is a procedure to extract the instrumentation (screws, rods or plates) implanted in a previous surgery, once the vertebral fusion has consolidated and the hardware is no longer required for stability. Many patients consider this option after months or years of localised pain over the screws, palpable prominence under the skin, hardware intolerance or suspected titanium allergy. Others present in the context of late infection or loosening that forces removal. This guide is written as a second opinion: the decision to remove the hardware is not always straightforward and depends on the real state of the fusion, the symptoms and the risks of operating again over the previous scar.
What is spine hardware removal?
Spine hardware removal is a procedure to extract previously implanted instrumentation — pedicle screws, rods, plates or hooks — once the vertebral fusion has consolidated and the hardware no longer plays an essential structural role. The approach is usually performed through the previous surgical scar.
Not every spinal implant should be removed: in many patients the hardware is well tolerated lifelong. Removal is considered when there are symptoms attributable to the implant (local pain over the screws, prominence, intolerance, late infection) or suspicion of loosening or titanium allergy. When fusion is NOT consolidated or there is broken hardware or pseudarthrosis, the right option is not simple removal but a failed instrumentation revision. To review your case, you can request a second opinion with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from hardware removal typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
Before considering removal, fusion consolidation is confirmed on CT and previous imaging, operative reports and dynamic radiographs are reviewed. If allergy is suspected, an allergological work-up is coordinated; if infection is suspected, blood tests with inflammatory markers and, when relevant, a bone scan are requested. Fasting instructions, medication adjustments and antibiotic prophylaxis are provided.
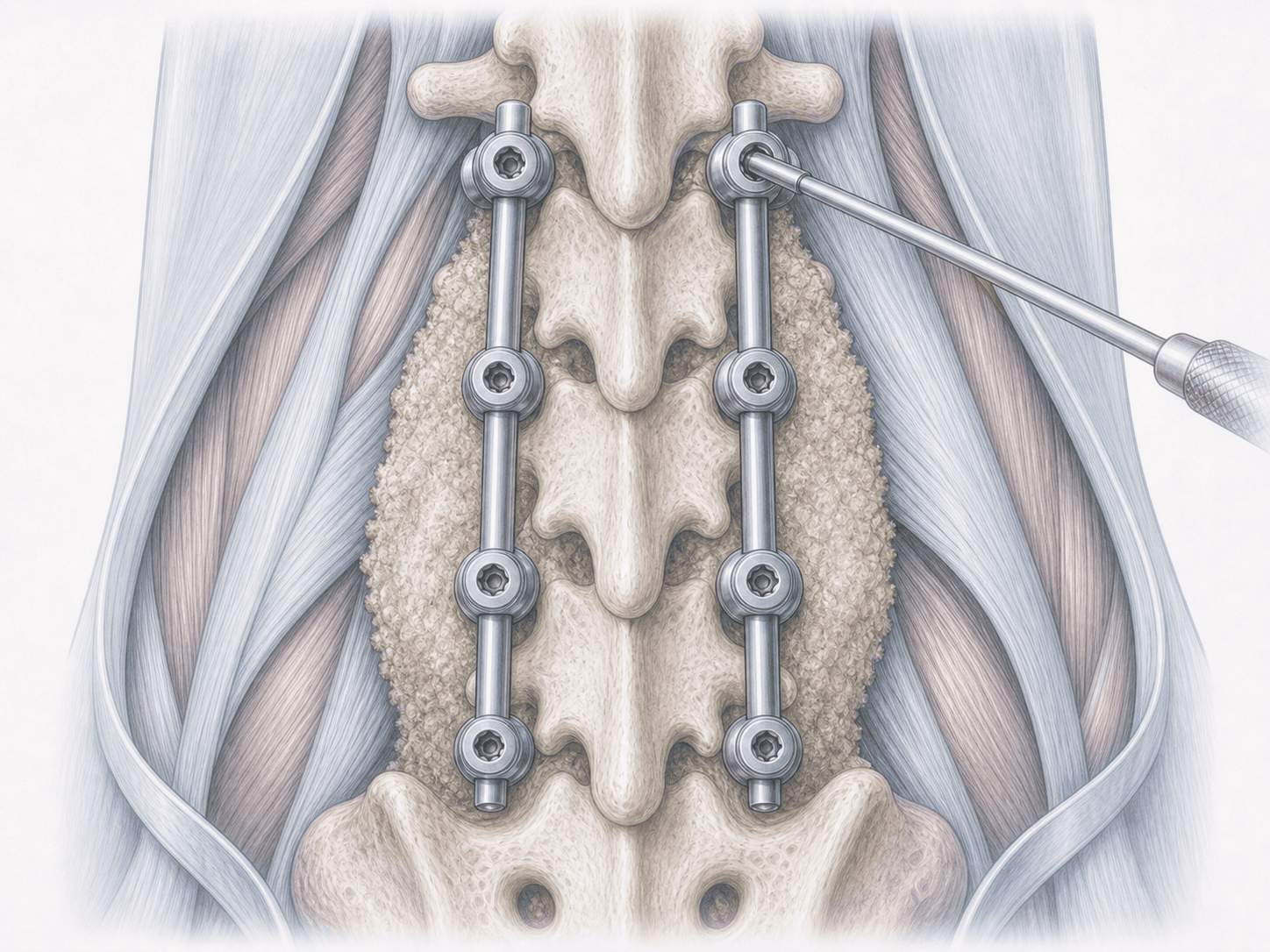
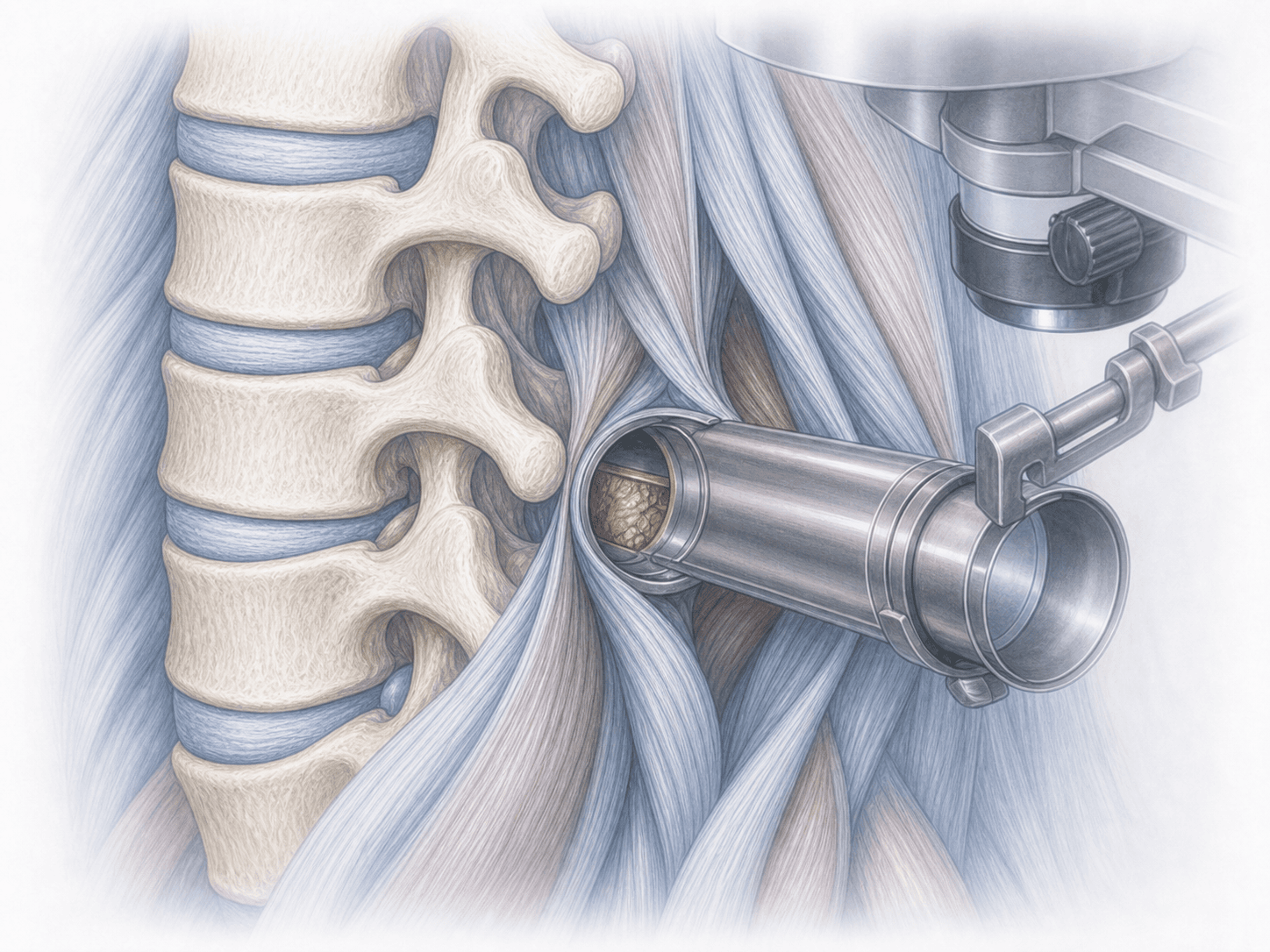
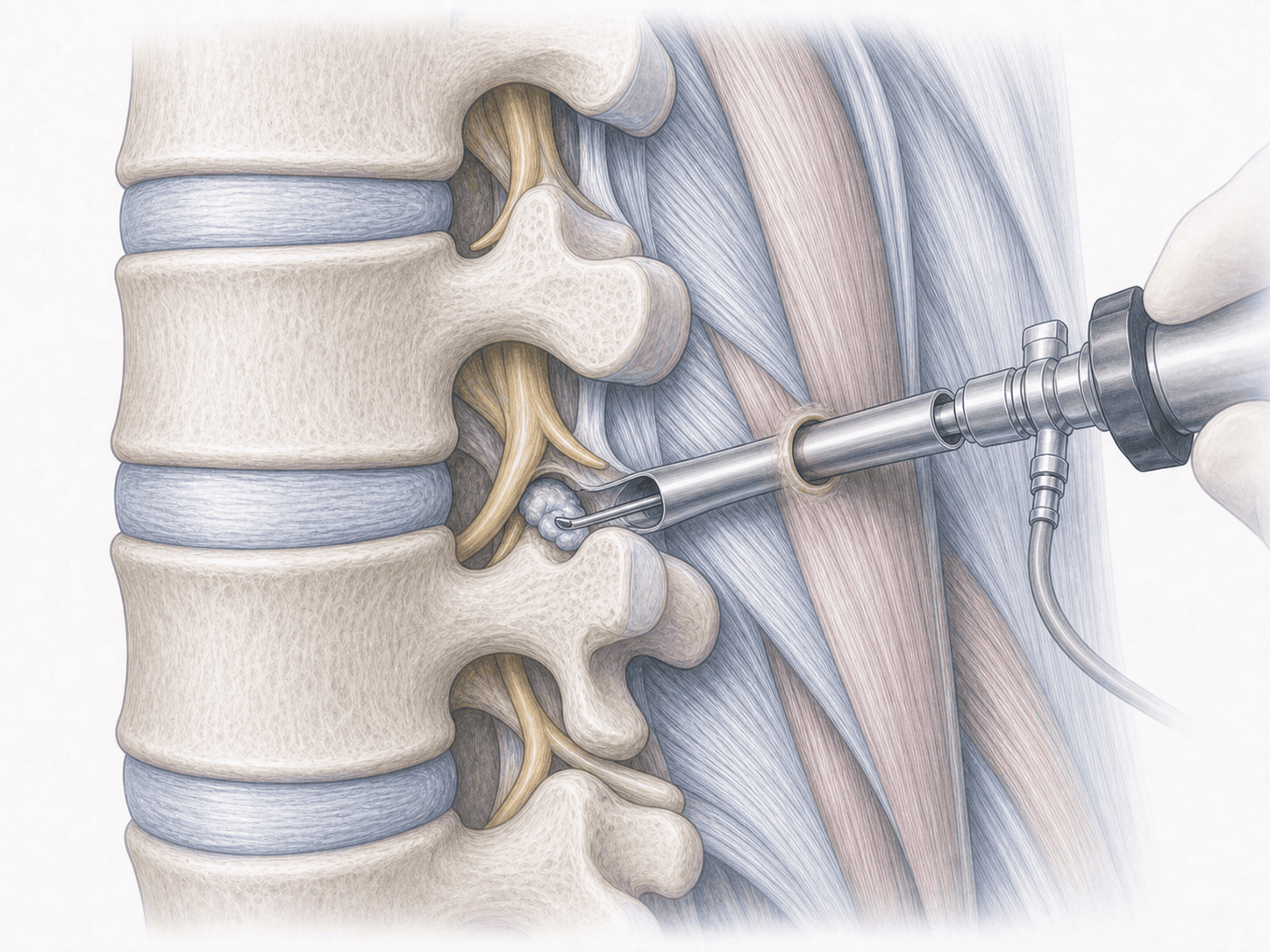
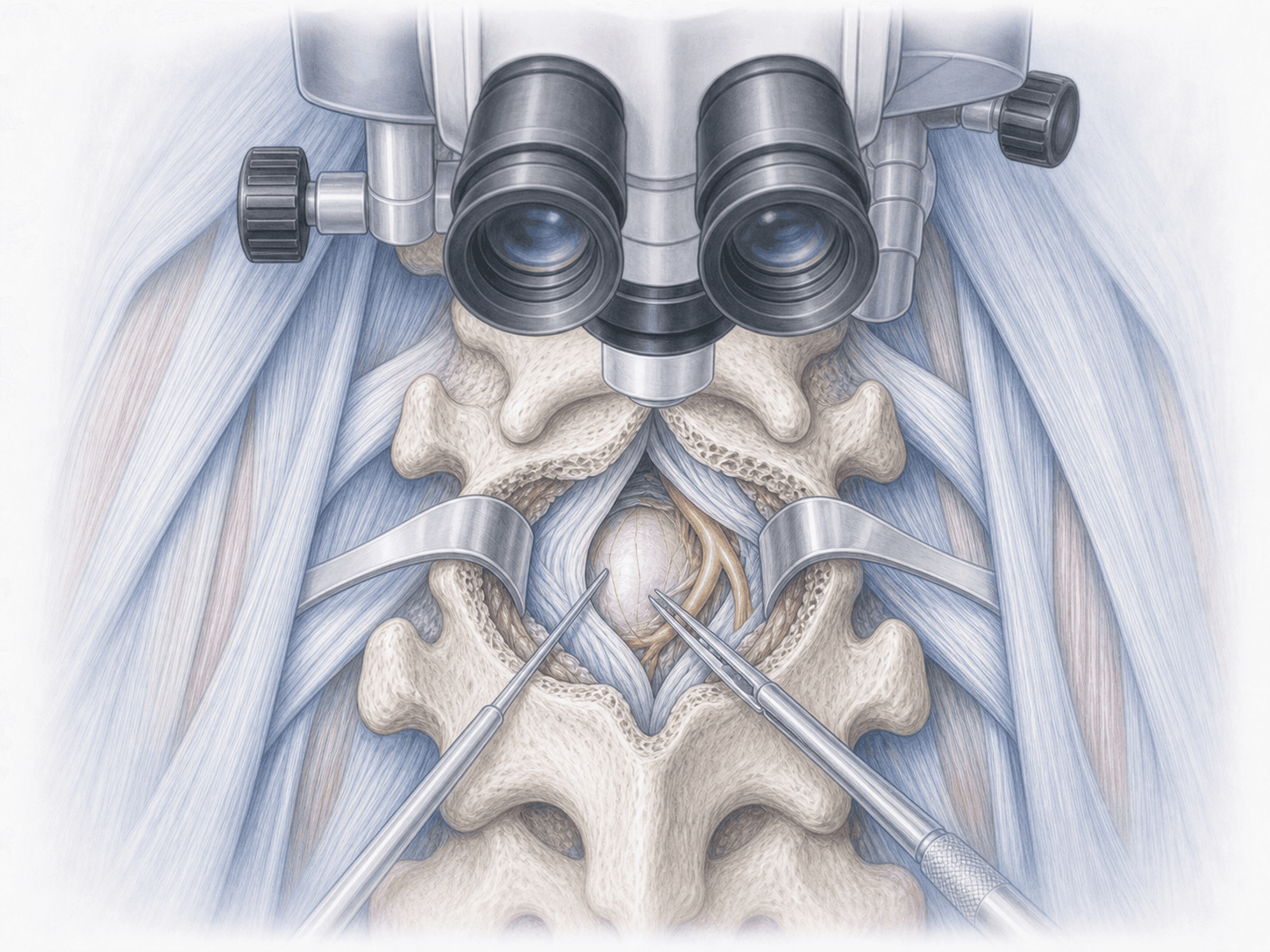
2.During the procedure
Surgery is performed under general anaesthesia. The spine is approached through the previous surgical scar; scar tissue is carefully identified and the hardware is located. Connectors, rods and screws are removed one by one under fluoroscopic guidance. If infection is detected, tissue samples are taken for culture and the area is debrided. Closure is performed in layers, respecting the original scar.
3.Immediate postoperative period
After surgery patients spend a short time in recovery before returning to their room. Pain is controlled, mobilisation begins progressively and the surgical wound is monitored. Hospital stay is usually 24–48 hours, longer if surgery was performed for infection or loosening.
Recovery after spine hardware removal
Recovery is usually faster than after the original surgery, because the segment is already fused and there is no need to protect a new arthrodesis. Daily activities resume within a few days and office work between 1 and 3 weeks, depending on the extent of the removed hardware and the quality of the scar tissue.
During the first weeks, heavy strain should be avoided to allow deep tissue healing. Physiotherapy is reintroduced gradually. Fever, wound discharge, new severe pain or any neurological symptom warrant immediate medical review.
Risks and possible complications
Any surgery through a previous scar carries general risks such as infection, bleeding, thrombosis or anaesthesia-related issues, which may be slightly higher than in primary surgery due to scar tissue.
Specific risks include nerve root or dural injury with cerebrospinal fluid leak, screw breakage during extraction that may require leaving fragments behind, persistence or recurrence of pain if the hardware was not the true source, and the appearance of instability if the fusion was less consolidated than imaging suggested. These risks are assessed individually.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala