Sacroiliac radiofrequency rhizolysis
Sacroiliac radiofrequency rhizolysis is a minimally invasive technique for patients with persistent sacroiliac pain who have already responded clearly to [diagnostic sacroiliac blocks](/en/treatments/sacroiliac-joint-blocks). The goal is to switch off the sensory branches that carry pain from the joint to the brain, without entering the joint itself and without affecting strength or gait. Relief typically lasts between 6 and 12 months and can be repeated if pain returns. This guide explains when it makes sense to consider it, how the session works step by step and what realistic results to expect.
What is sacroiliac radiofrequency rhizolysis?
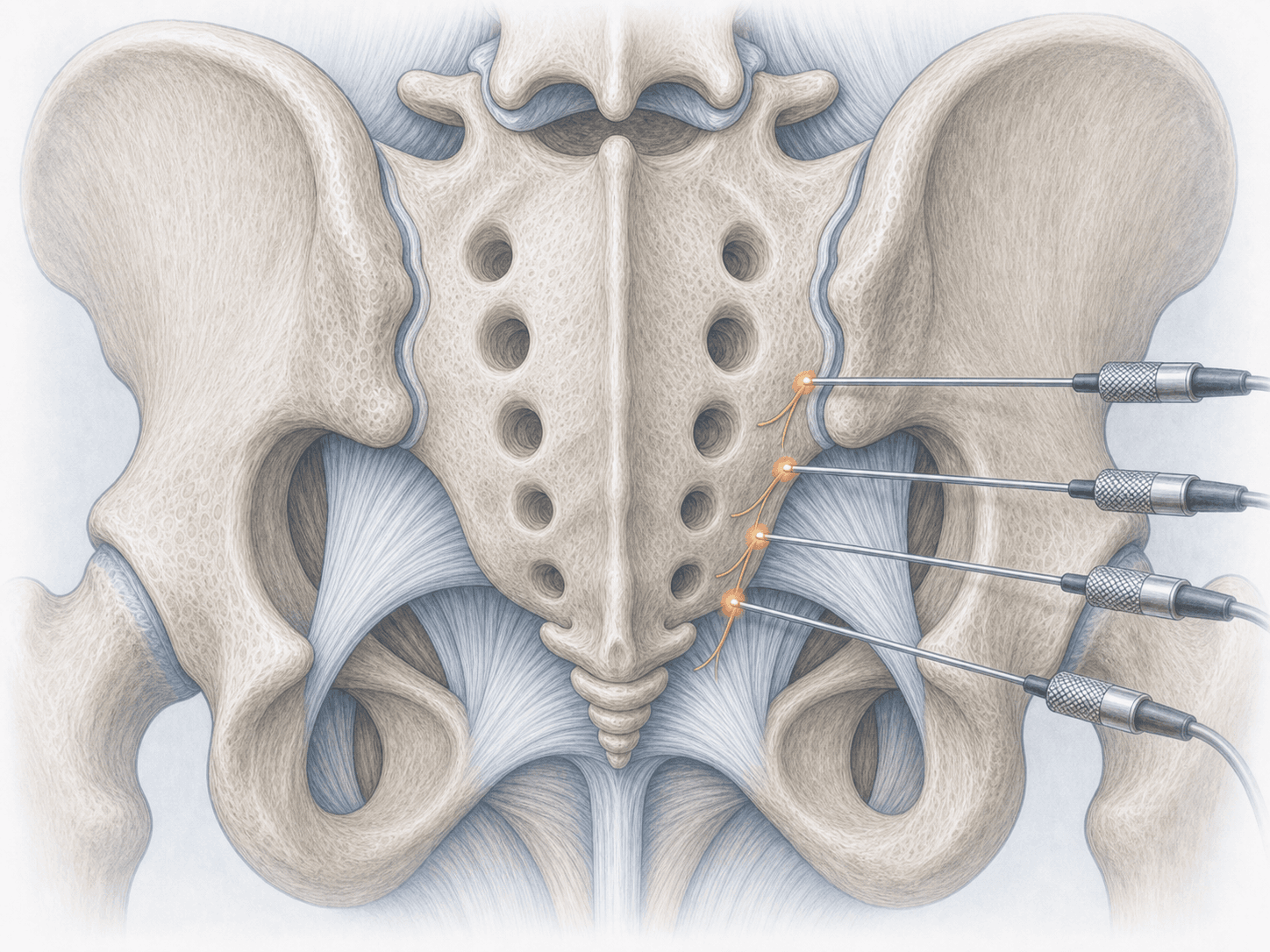
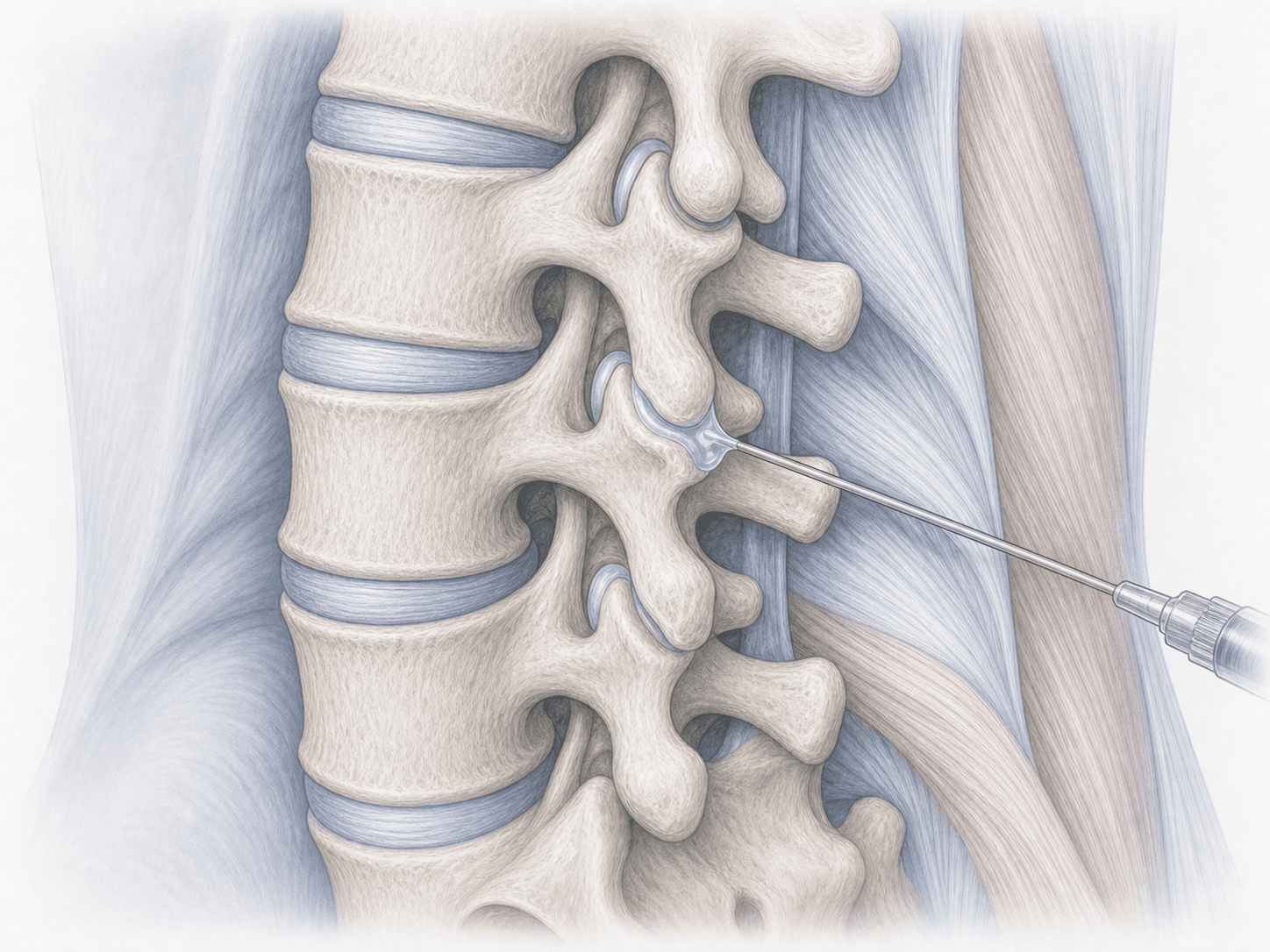
Sacroiliac radiofrequency rhizolysis, also known as sacroiliac denervation or neurotomy, is a fluoroscopy-guided percutaneous procedure that applies controlled heat to the sensory branches that innervate the joint. The lateral dorsal branches of S1, S2 and S3 are usually treated, often combined with the L5 dorsal ramus, because this is the nerve network that carries pain from the posterior aspect of the joint.
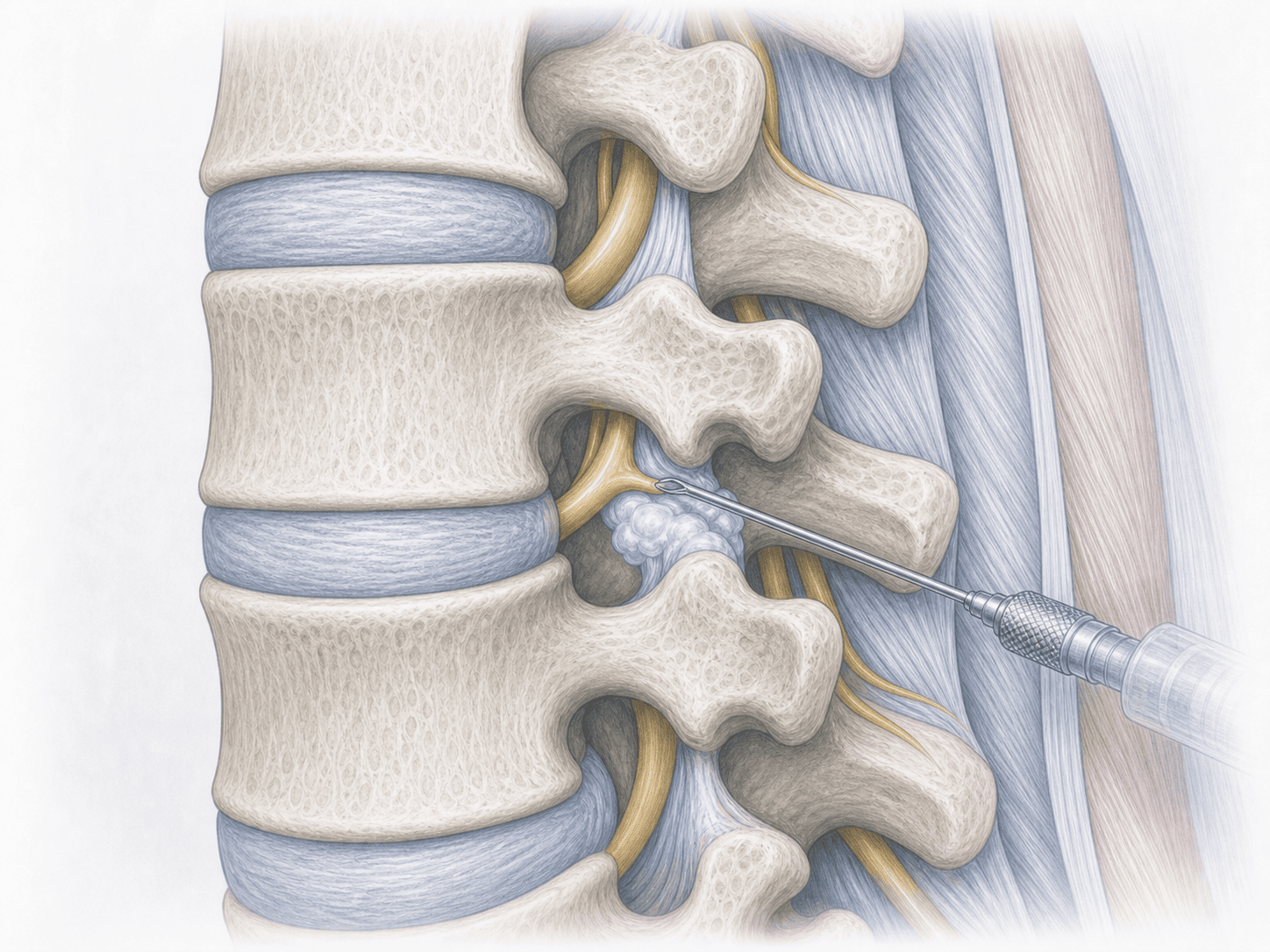
The technique can be performed with conventional radiofrequency, cooled radiofrequency or bipolar strip lesions. They all share the same logic: create a thermal lesion large enough to interrupt the pain signal for months, without touching the joint itself, the spinal cord, or affecting strength or sphincter control.
It is only indicated when diagnostic sacroiliac blocks have been clearly positive, meaning they have reproduced and reliably relieved the pain. To discuss your case you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit usually describe a fairly specific pattern:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
Before the session we review prior diagnostic blocks, MRI and current medication. If you take anticoagulants or antiplatelet drugs, they are adjusted according to protocol. Light fasting for a few hours is required and same-day discharge is planned. The procedure is performed under local anaesthesia and light sedation; general anaesthesia is not needed in most cases.
2.During the procedure
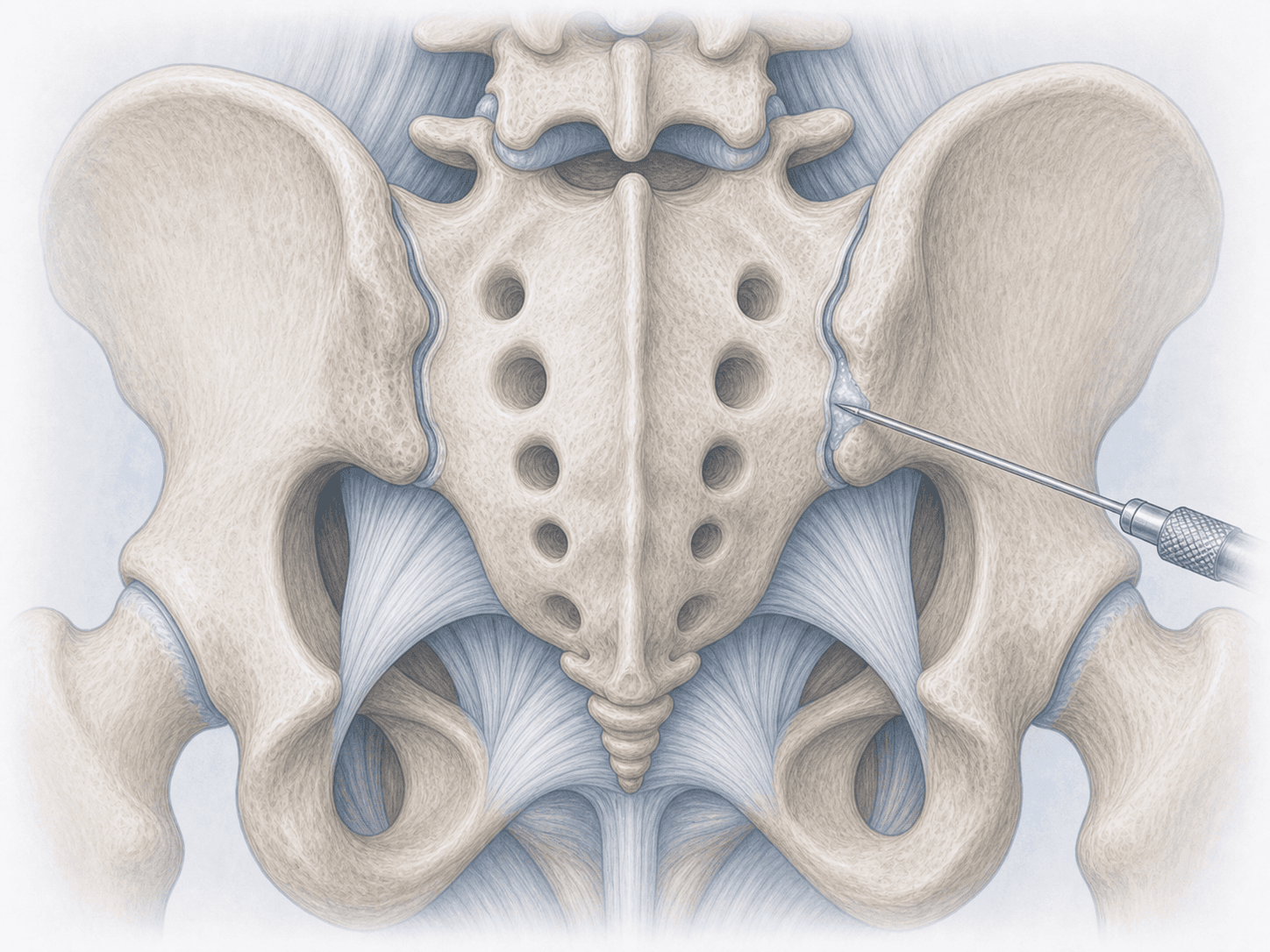
The patient lies prone on the table with the lumbosacral area prepared sterilely. Under fluoroscopy the sacral foramina and the L5-sacrum junction are identified. Electrode needles are introduced at the L5 dorsal ramus and the lateral branches of S1, S2 and S3.
Before applying radiofrequency, sensory and motor stimulation tests confirm that the electrode is close to the sensory nerve and not to a motor nerve. Controlled heat is then delivered (conventional, cooled or bipolar strip radiofrequency) for several minutes per point. The whole session usually takes between 45 and 75 minutes.
3.Immediate postoperative period
After the session you stay under observation for one to two hours. Local soreness or discomfort for the first 3-7 days, sometimes longer, is common, because the thermal lesion produces transient nerve irritation before its definitive effect. Real relief is not immediate: it builds progressively between weeks 2 and 4. Same-day discharge is the rule, with local cold for the first two days and gradual return to normal life.
Recovery and realistic outcomes
Return to everyday activity is usually quick: walking, driving or office work resume within a few days. Impact sports, lifting significant weights and sustained postures are reintroduced between weeks 2 and 3 depending on how the area feels.
Meaningful relief of sacroiliac pain establishes between weeks 2 and 6 and typically lasts 6 to 12 months, sometimes longer. It is not a permanent cure: sensory nerves regenerate over time and, if pain returns, the procedure can be repeated with usually similar results. The relief window is the right moment to reinforce the trunk and pelvic stabilising muscles, which are what protect the long-term outcome.
If at any point fever, disproportionate pain, leg weakness or sphincter changes appear, you should reach out for review.
Risks and possible complications
Sacroiliac radiofrequency rhizolysis has a favourable safety profile, but it is not risk-free.
The most common issues are mild and transient: pain at the puncture site for the first few days, a burning or tingling sensation over the sacrum and, occasionally, a small haematoma. Less frequent risks include unintended injury to a motor branch (unlikely thanks to prior stimulation testing), a patch of skin numbness over the sacrum or buttock, post-rhizolysis neuritis with more intense pain for 1-2 weeks and puncture-site infection, which is very rare.
More important than these risks is another realistic possibility: that the relief is smaller than expected or shorter than hoped. Strict selection through diagnostic blocks beforehand is the main tool to minimise this scenario.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala