Facet radiofrequency rhizotomy
Facet radiofrequency rhizotomy is a minimally invasive procedure aimed at relieving chronic low back (or neck) pain that arises from the facet joints of the spine. It is intended for patients with mechanical pain that clearly and temporarily improves after prior diagnostic facet blocks, and in whom conservative measures are no longer enough. This guide explains in plain terms what to expect before, during and after the procedure, including how long relief typically lasts and what to do if pain returns.
What is facet radiofrequency rhizotomy?
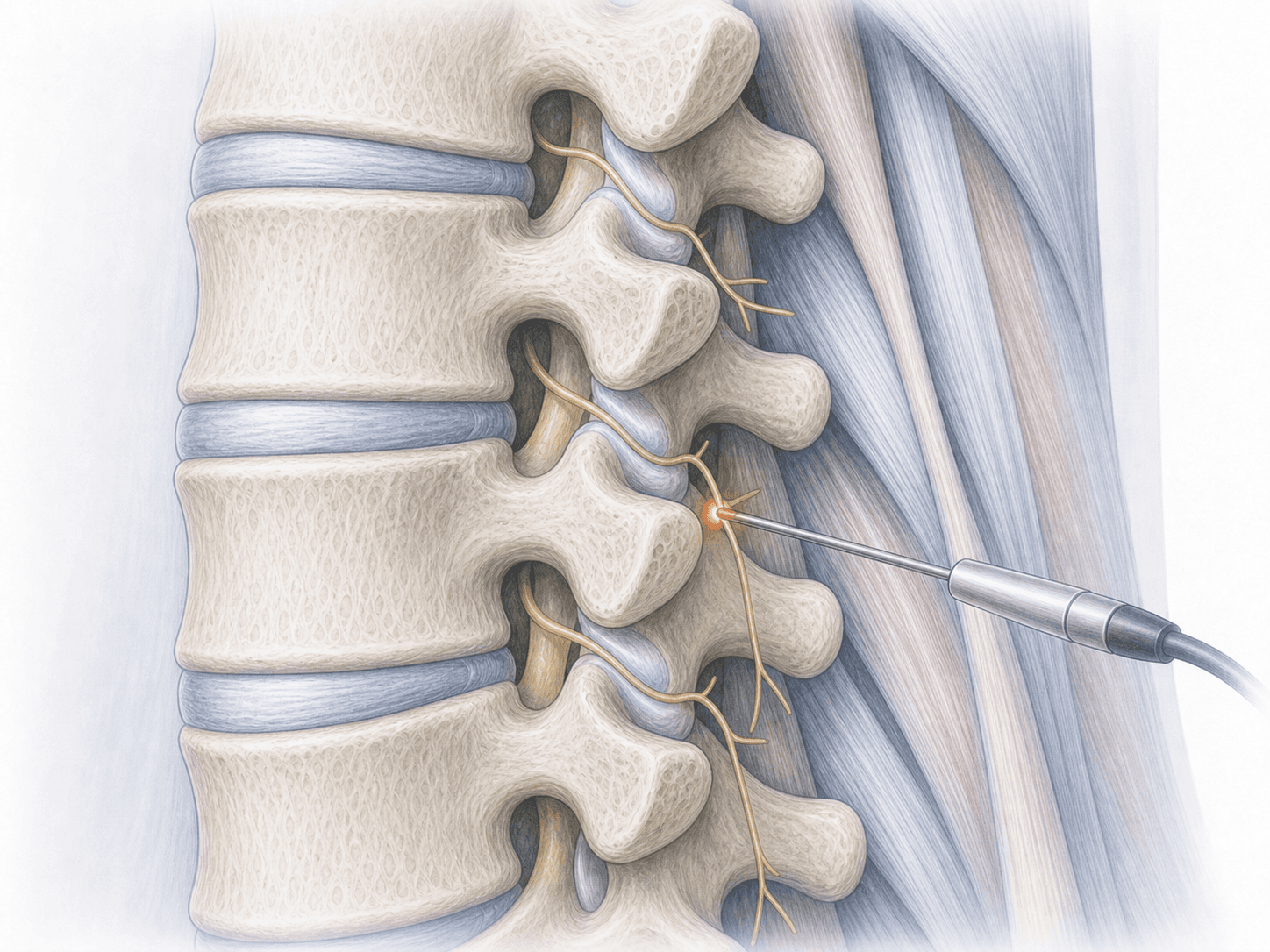
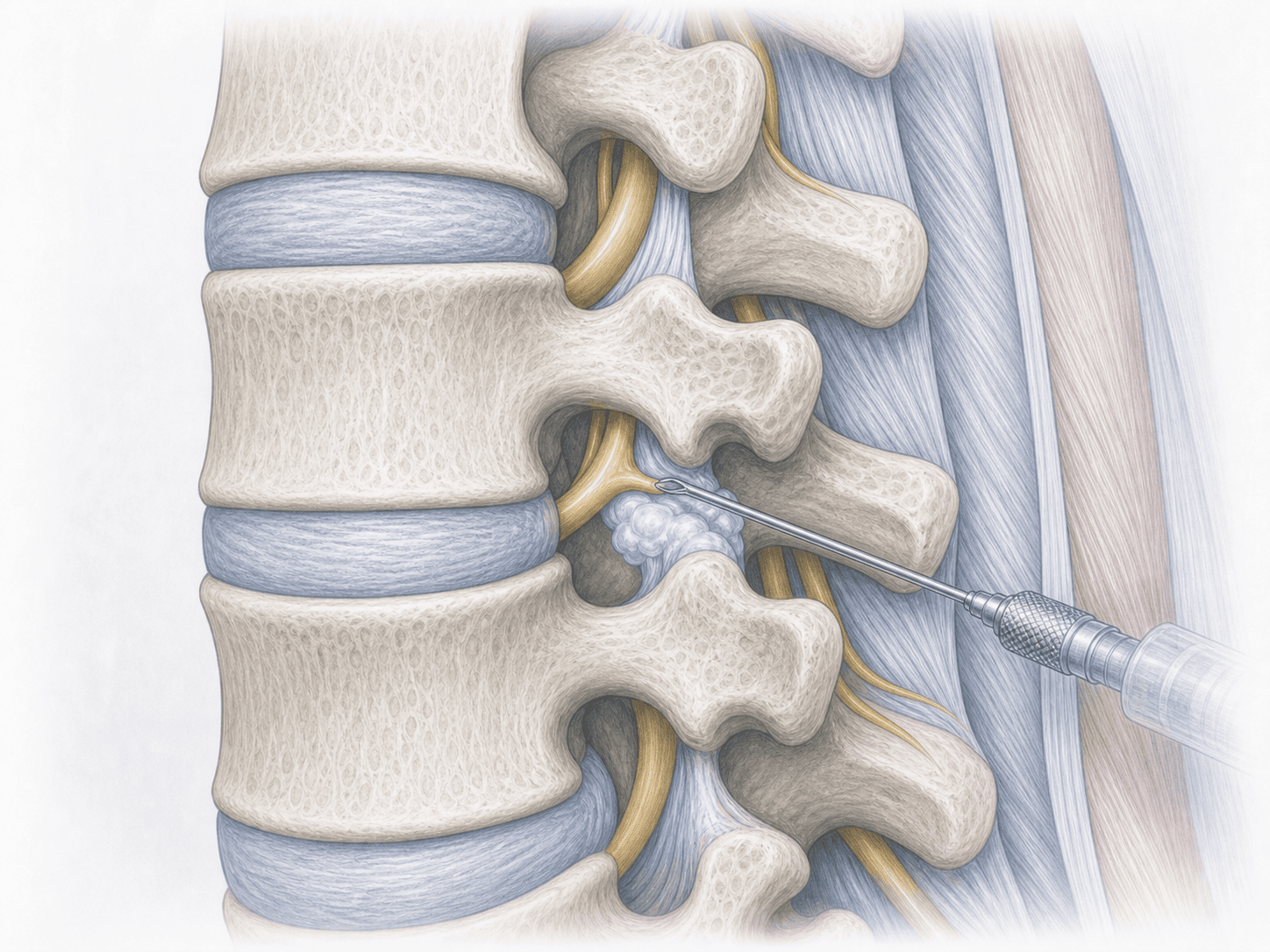
Facet radiofrequency rhizotomy (also called medial branch neurotomy or facet denervation) is a percutaneous, fluoroscopy-guided procedure in which heat is applied through a radiofrequency electrode onto the medial branch of the dorsal ramus. This small nerve carries pain signals from the facet joint; interrupting it reduces mechanical back pain.
Unlike facet joint blocks, which mainly serve to confirm the diagnosis, rhizotomy aims at longer-lasting relief, typically 6 to 12 months, in patients whose diagnostic blocks have been positive. To check whether your case fits, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from facet rhizotomy typically report:
When is facet rhizotomy indicated?
How is the procedure performed?
1.Preoperative preparation
Preparation includes confirming that diagnostic facet blocks were clearly positive, reviewing imaging and current medication (especially anticoagulants and antiplatelets) and answering any questions. Light fasting instructions are given, and the procedure is planned either under local anaesthesia with mild sedation or under local anaesthesia alone.
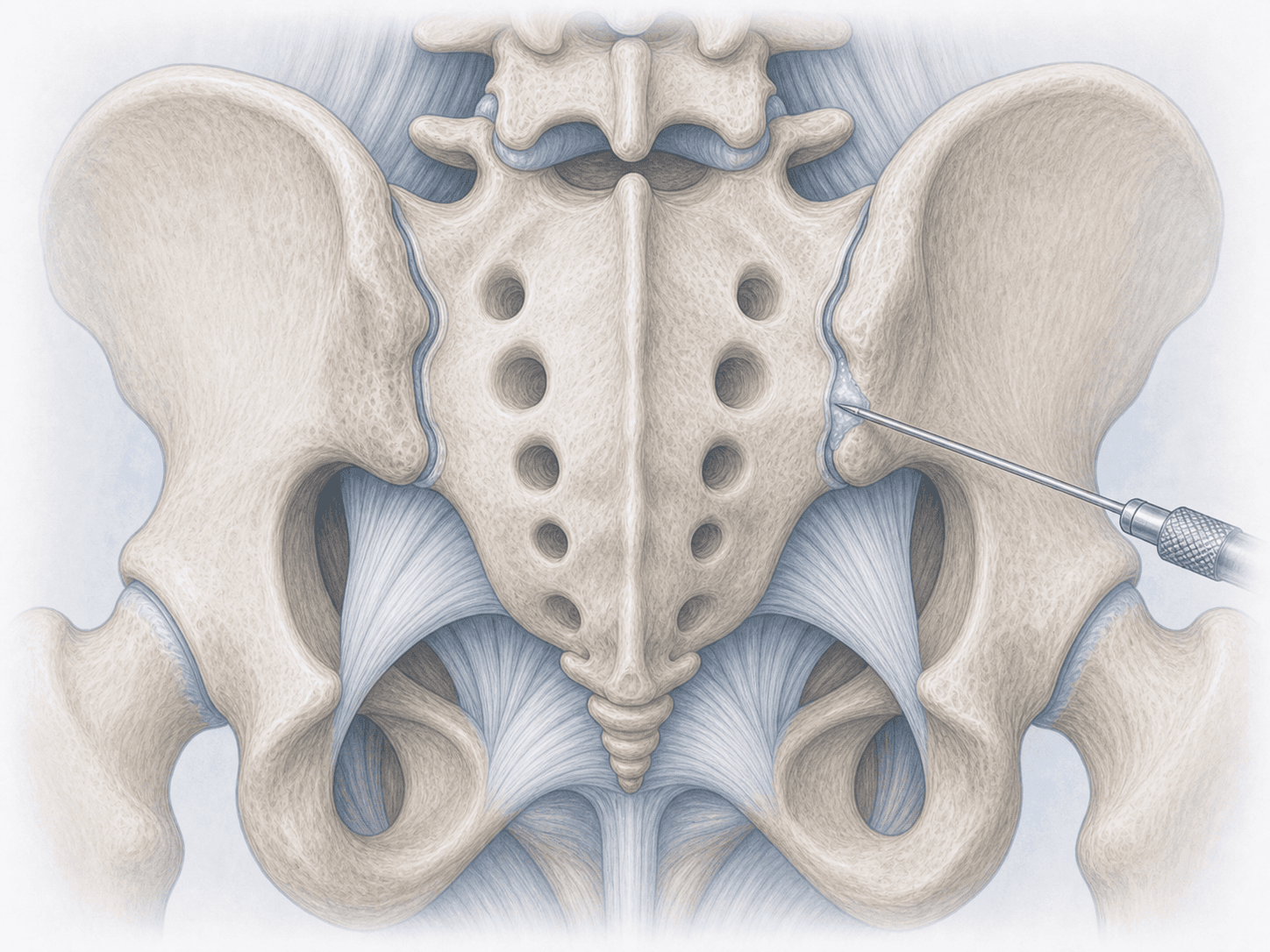
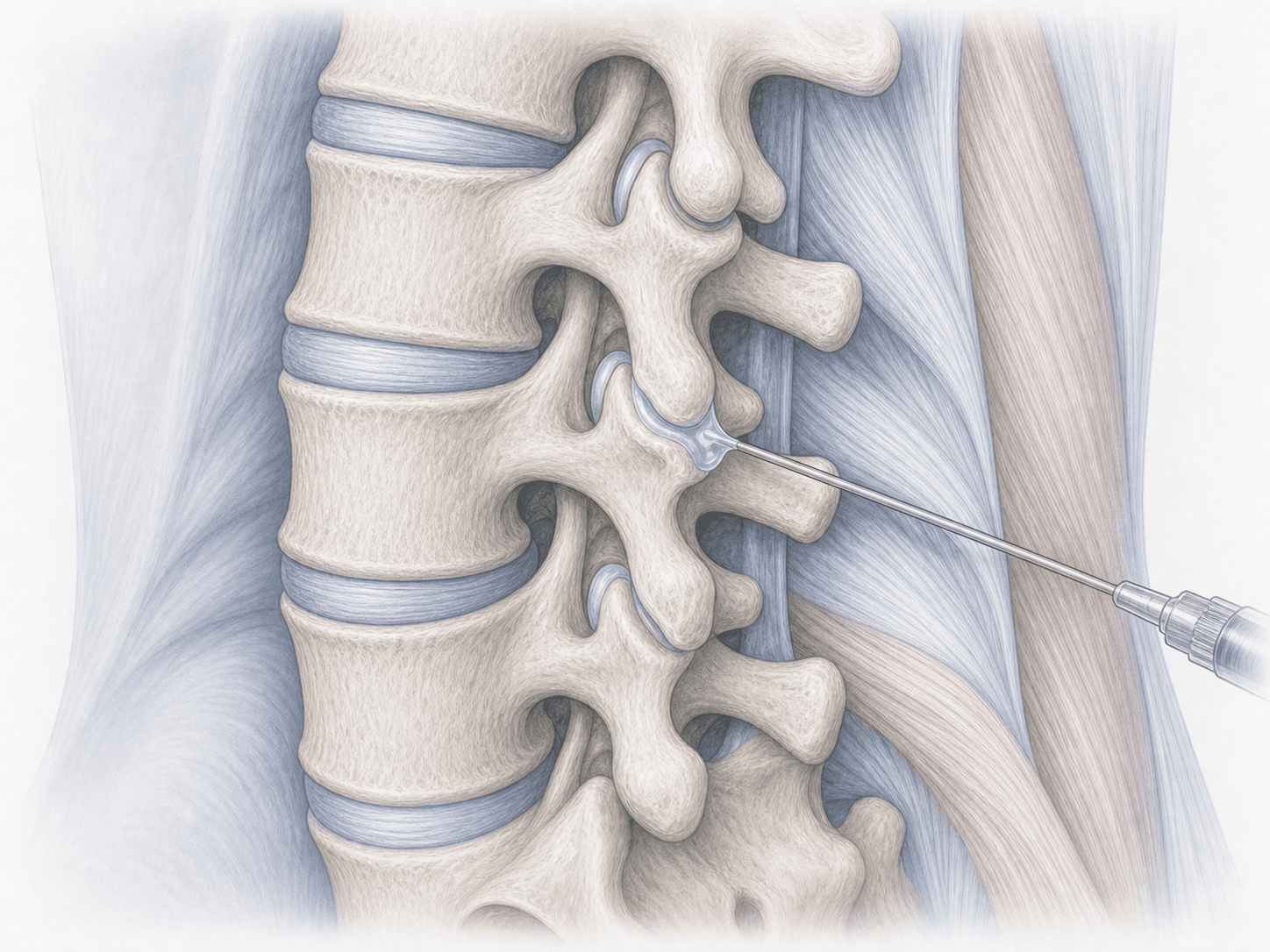
2.During the procedure
The patient lies prone on the table. Under fluoroscopic guidance the target facet levels are identified and thin cannulas are advanced onto the medial branch. Before applying radiofrequency, sensory and motor stimulation are performed to confirm correct targeting and rule out proximity to a nerve root. Controlled heat is then delivered (typically 80-90 °C for 60-90 seconds) at each level. The whole procedure usually takes 30-60 minutes depending on the number of levels treated.
3.Immediate postoperative period
After the rhizotomy the patient is monitored for a short period. Local tenderness in the treated area for a few days is common, and a temporary mild flare-up of the usual pain may occur before improvement, related to the controlled thermal lesion itself. Most patients go home the same day and resume light activity within 24-48 hours.
Recovery after facet rhizotomy
Recovery is quick. Daily activities are usually resumed the next day and office work within a few days. Intense effort and impact sports should be avoided for 1-2 weeks.
Pain relief is not always immediate: a gradual improvement over 2-4 weeks is common as the treated tissue heals. The effect typically lasts 6 to 12 months, a window that is best used for physiotherapy and core strengthening. If pain returns with the same mechanical pattern, rhizotomy can be repeated with good results.
Risks and possible complications
Facet rhizotomy is a low-risk procedure, but it is not free of complications.
The most common issues are: local discomfort or burn-like soreness at the puncture site, a transient flare-up of pain in the first days, superficial bruising and mild infection (uncommon). Rarely, temporary involvement of a nearby nerve root can cause dysesthesia or mild weakness, which is why prior stimulation is performed. It must also be accepted that in some patients relief is less than expected or shorter, or that pain returns before 6 months.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala