Endoscopic lumbar discectomy
Endoscopic lumbar discectomy is the most minimally invasive version of lumbar disc herniation surgery. Through a 7-8 mm incision, we introduce an endoscope with a camera that allows us to remove the herniated fragment under direct vision, preserving the paraspinal muscles and the rest of the healthy disc. Many patients come to our clinic after months of sciatica that has not improved with physiotherapy, medication or injections. They look for an effective solution, but also a fast recovery that allows them to get back to their lives soon. This guide explains how the procedure works, which herniations it is indicated for and what to expect before, during and after, so you can make an informed and calm decision.
What is endoscopic lumbar discectomy?
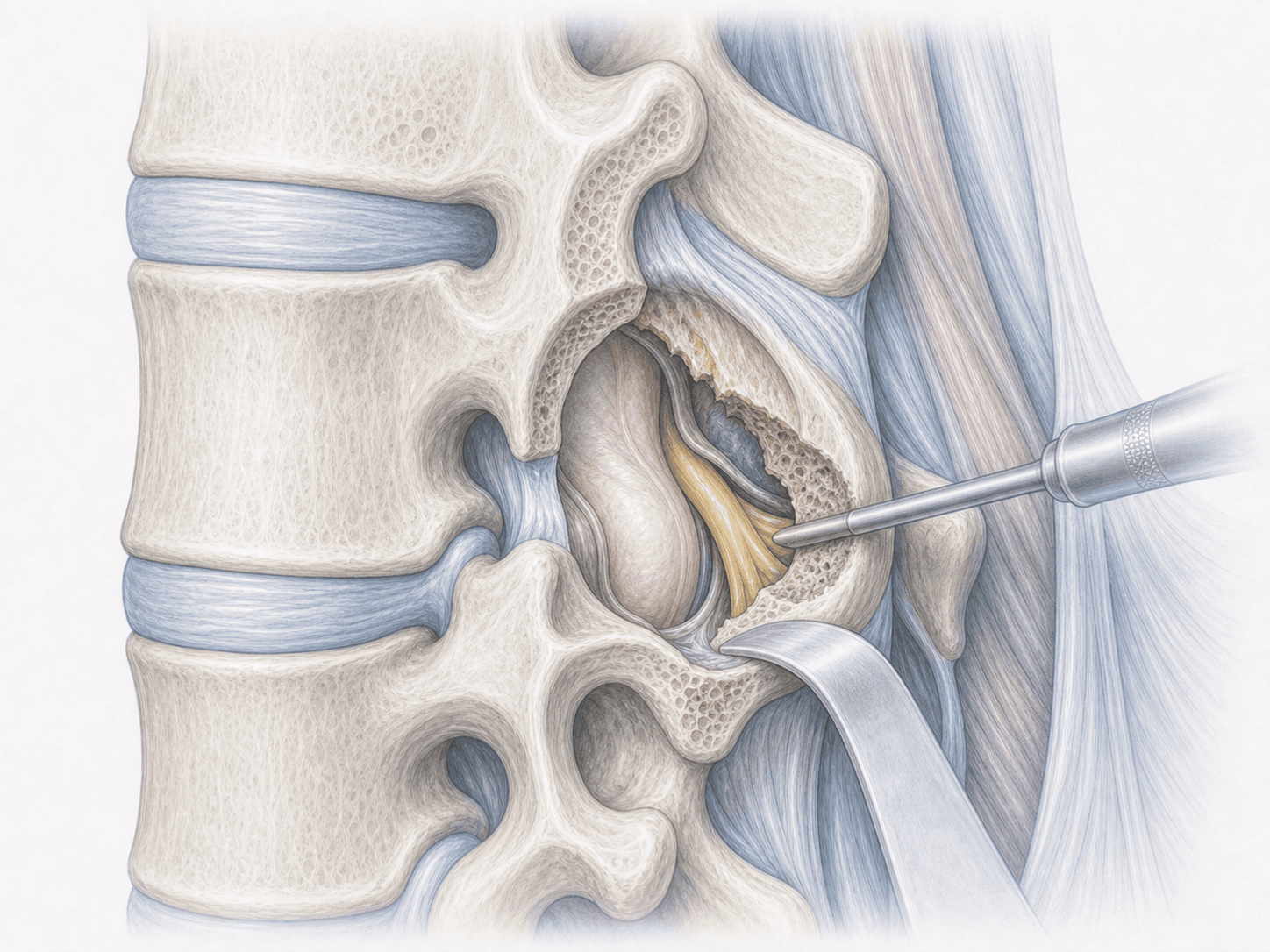
Endoscopic lumbar discectomy is a minimally invasive procedure that removes the herniated disc fragment compressing a lumbar nerve root through a 7-8 mm incision, under direct endoscopic vision. We usually perform it under local anaesthesia with sedation, which allows same-day discharge in most patients.
There are two main approaches: the transforaminal (TESSYS), which enters laterally through the foramen and is ideal for foraminal and extraforaminal herniations; and the interlaminar (Iprime), which enters through the posterior midline, particularly useful at L5-S1 when the pelvis makes lateral access difficult.
Compared with classical lumbar microdiscectomy, it offers the same efficacy on sciatic pain with less muscle injury, less bleeding and a faster recovery. If you want to know whether your herniation is a candidate, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from endoscopic lumbar discectomy typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
We review together the MRI and the clinical examination to confirm the indication and choose the approach (transforaminal or interlaminar) according to the location of the herniation. We provide fasting instructions of 6-8 hours, adjustment of any anticoagulant medication and tailored recommendations for an outpatient procedure. We answer every question before signing the informed consent.
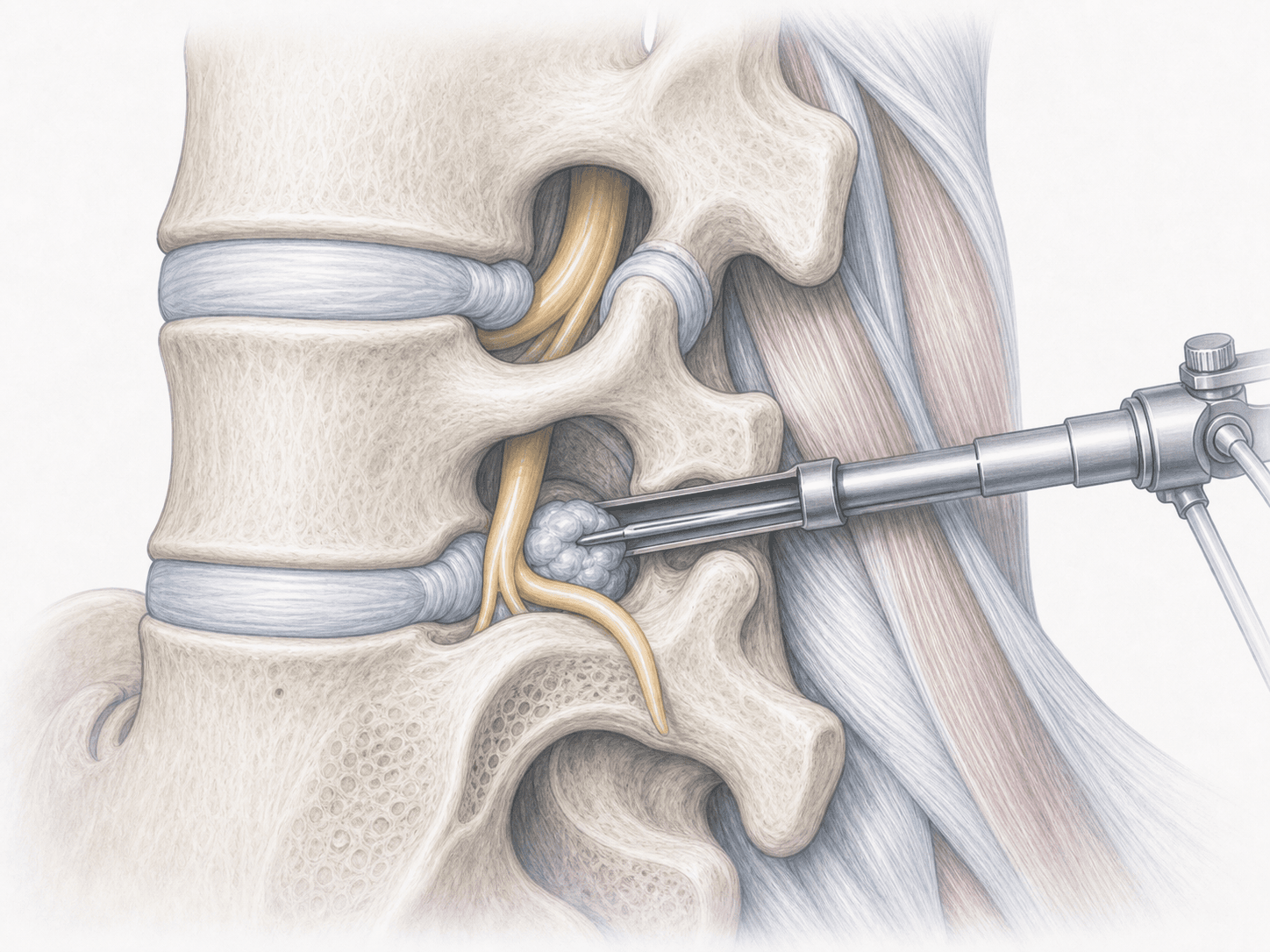
2.During the procedure
The patient is positioned prone. We usually use local anaesthesia with sedation, which allows some communication during surgery and adds neurological safety. We make a 7-8 mm incision and, guided by fluoroscopy, advance the endoscope with the camera to the herniation. Under direct vision, we remove the herniated fragment compressing the nerve root, preserving the paraspinal muscles and the healthy disc. Closure requires a single stitch and the procedure lasts between 45 and 90 minutes depending on the case.
3.Immediate postoperative period
After surgery, the patient spends a few hours in recovery. Most people stand up and walk the same day and are discharged within hours. We provide a clear plan of oral analgesia, wound care and activity guidance for the first days at home.
Recovery after endoscopic lumbar discectomy
Recovery is notably fast compared with open surgery. Daily activities are usually resumed within 3-7 days, office work around 1-2 weeks and physical jobs typically require 4-6 weeks depending on demands.
We recommend walking from day one in a progressive way, avoiding lifting and postponing impact sports during the first weeks. Rehabilitation, when indicated, usually begins between the second and fourth week. In case of fever, sudden increase in pain or new neurological deficits, you should contact us immediately.
Risks and possible complications
Every surgery involves general risks such as infection, bleeding or anaesthesia-related complications, although these are lower because the procedure is minimally invasive and usually performed without general anaesthesia.
Specific risks include recurrence of the herniation at the same level (around 5-7% in published series, comparable to microdiscectomy), transient nerve root injury with postoperative dysaesthesia, cerebrospinal fluid leak (uncommon) and, in selected cases, the need to convert to open surgery. Risks are assessed individually for each patient.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala