Minimally invasive lumbar fusion
Minimally invasive lumbar fusion (MIS) is a technique used to fuse one or more lumbar segments through small skin incisions, using percutaneous pedicular screws guided by fluoroscopy or intraoperative navigation. It is a useful option for grade I–II spondylolisthesis, degenerative instability or lumbar stenosis with instability, when pain or neurological symptoms have not improved with conservative treatment. Compared with classic open surgery, the MIS approach aims to preserve the paraspinal muscles, reduce blood loss and shorten recovery, while keeping the same surgical goals: decompression and stabilisation.
What is minimally invasive lumbar fusion?
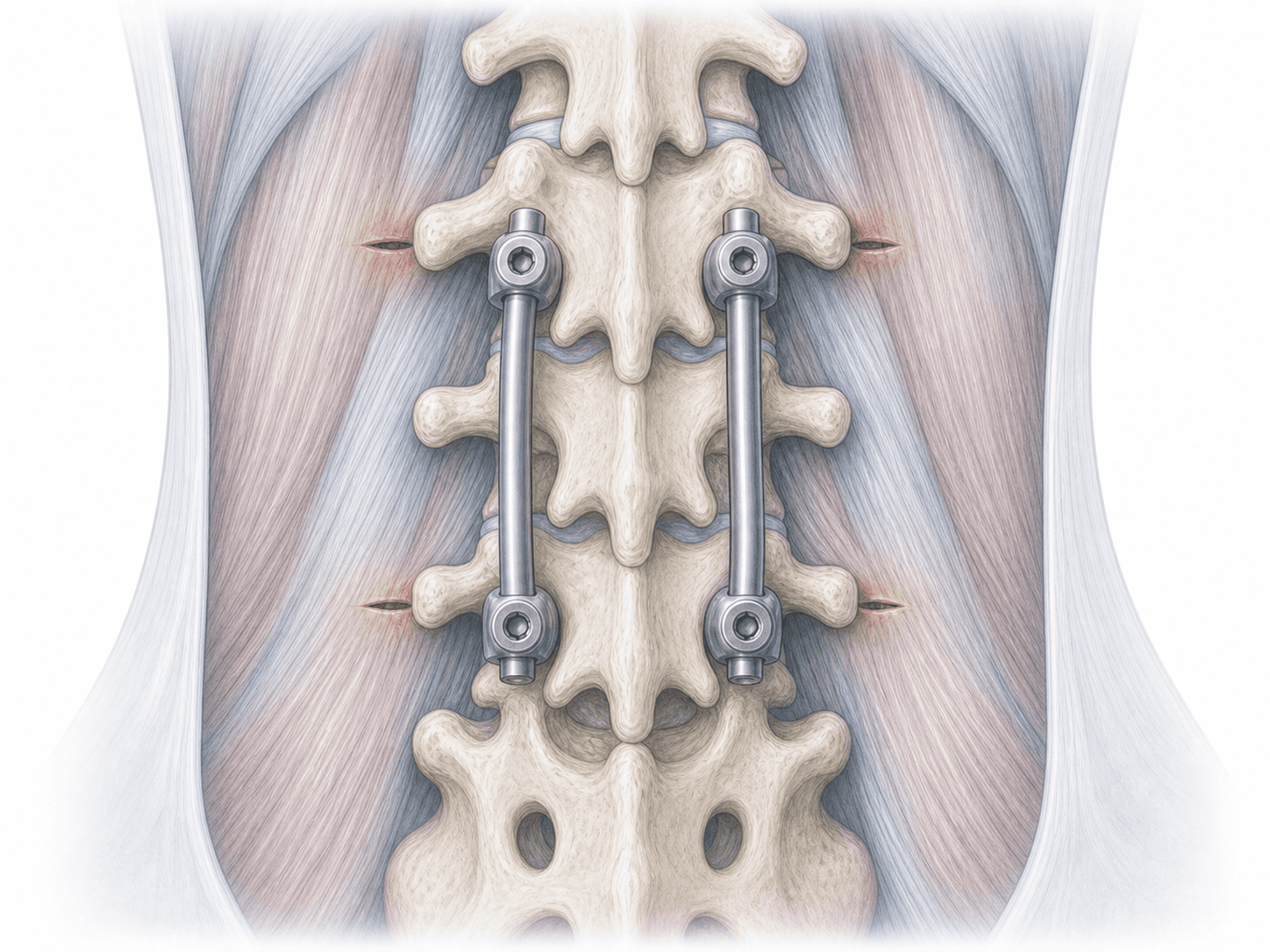
Minimally invasive lumbar fusion (MIS) is a procedure to fuse one or more lumbar segments through small skin incisions. The pedicular screws are placed percutaneously, guided by fluoroscopy or intraoperative navigation, and connected with rods to stabilise the segment while the bony fusion takes place.
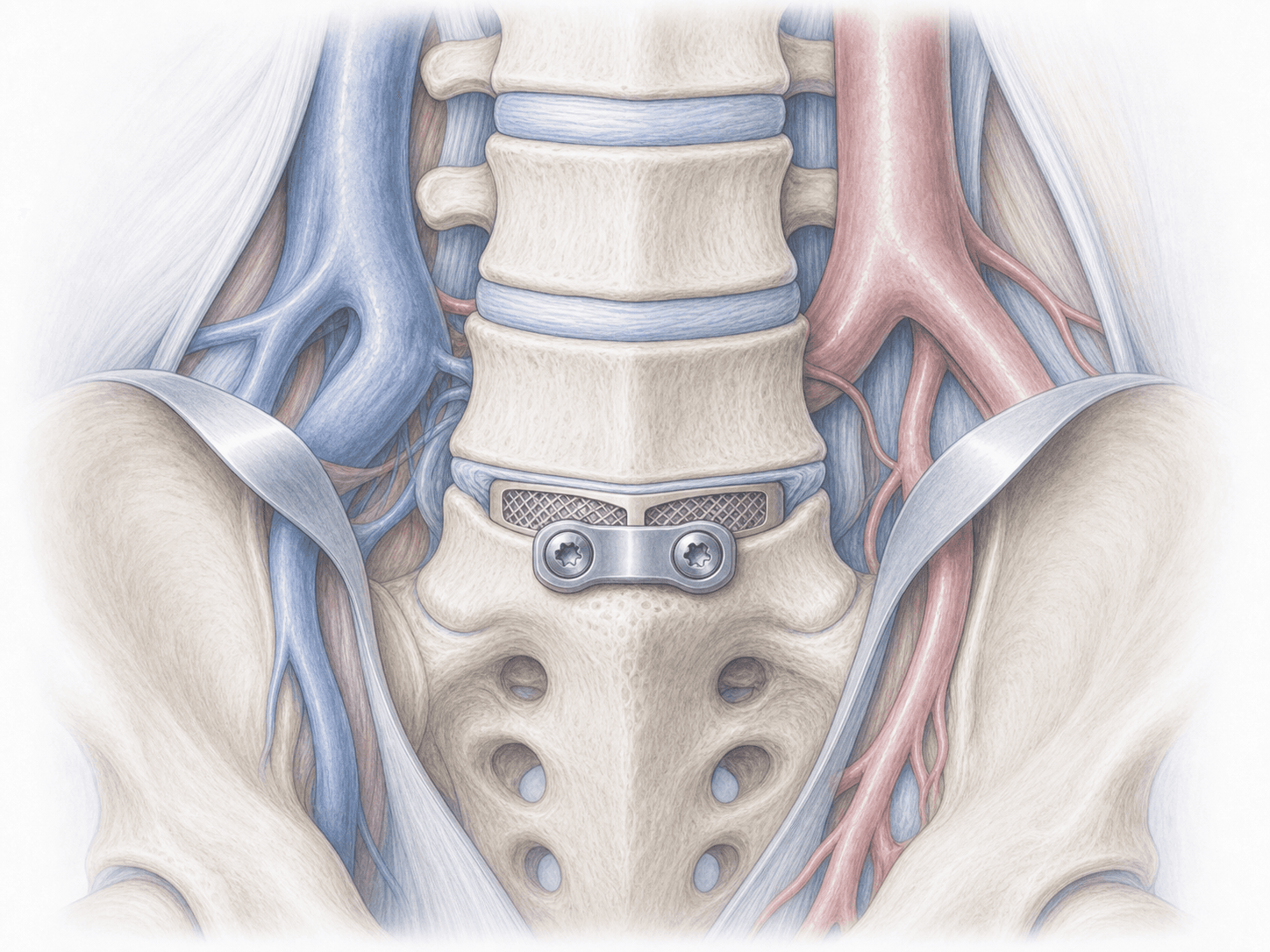
Unlike the traditional open approach, the paraspinal muscles are not stripped from the spine. This results in less blood loss, less postoperative pain and a faster return to daily activities. The technique is often combined with an interbody approach such as TLIF when nerve root decompression or restoration of disc height is also needed.
Not every patient is a candidate for MIS: the indication depends on the anatomy, the number of levels and the underlying pathology. To discuss your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from MIS lumbar fusion typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
Includes a detailed clinical assessment, MRI and dynamic X-ray review and planning of each screw trajectory on the imaging. Fasting instructions, medication adjustments (especially antiplatelets and anticoagulants) and case-specific recommendations are provided.
2.During the procedure
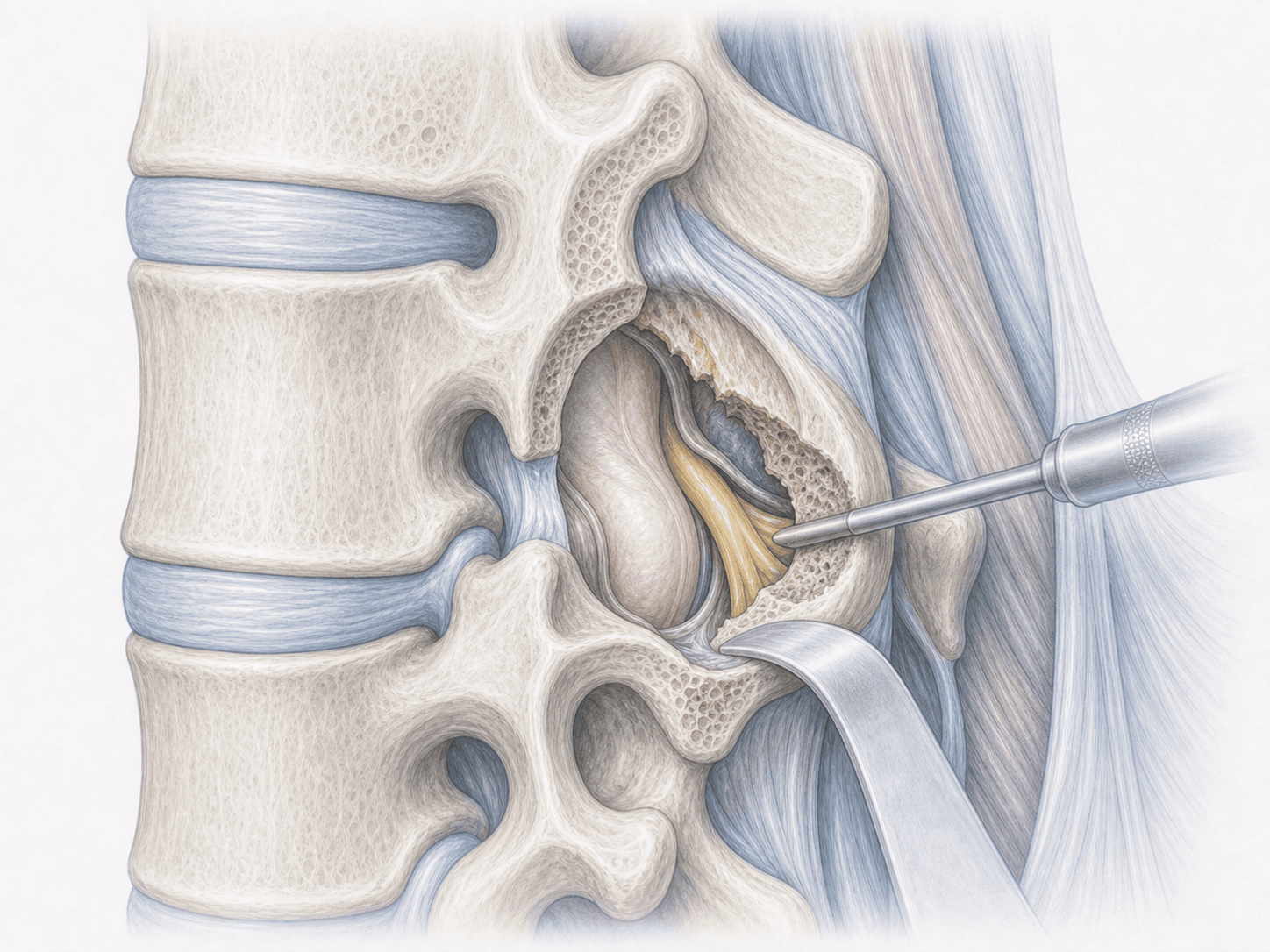
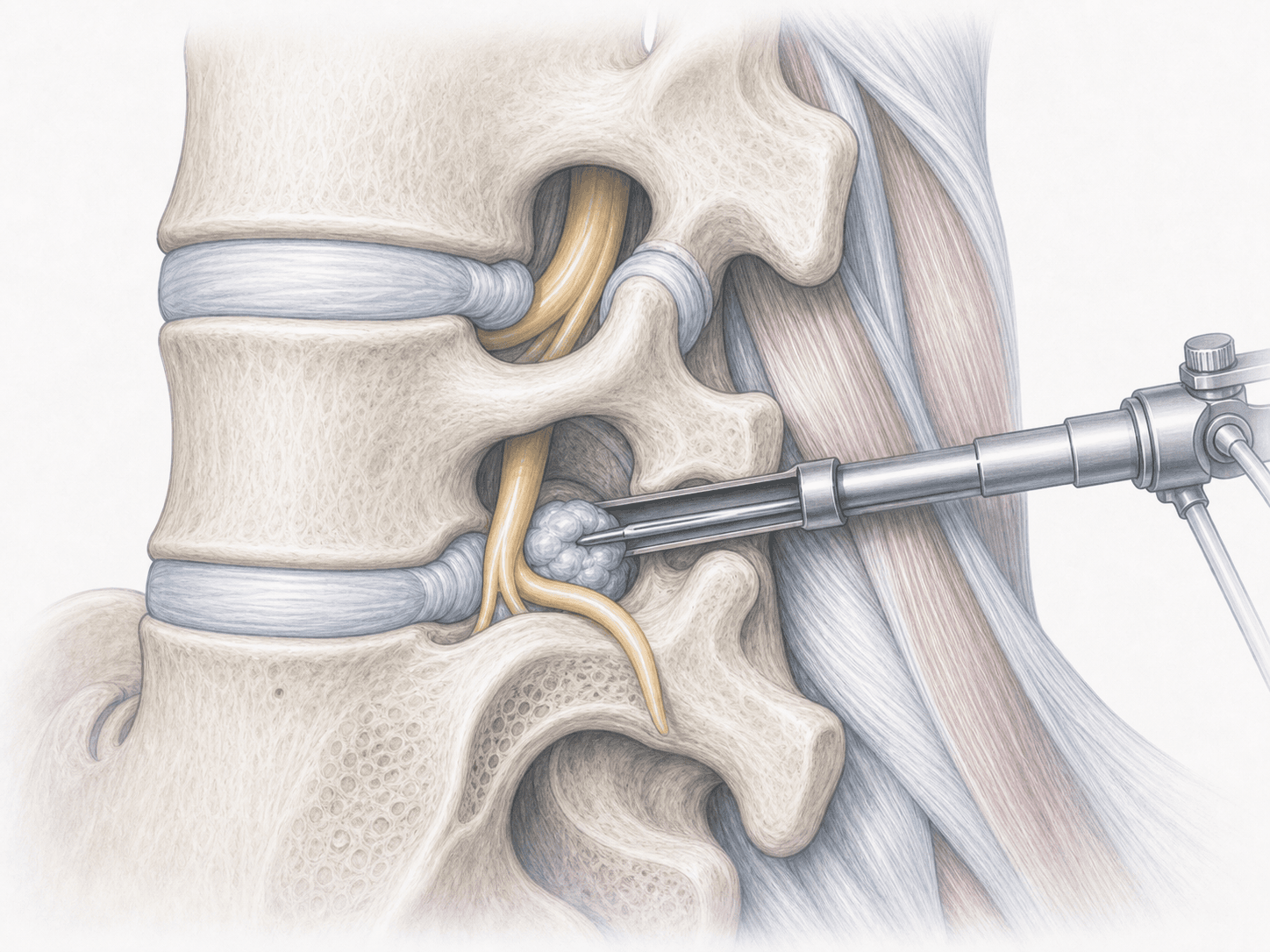
With the patient in the prone position under general anaesthesia, the pedicles are located with fluoroscopy or navigation. Through small incisions of about 1.5–2 cm on each side, needles and dilators are advanced to the pedicle and the percutaneous screws are placed. When indicated, a decompression or interbody approach (TLIF) is performed through one of the incisions to remove the disc and place a cage. Finally, the rods are passed through the screws and tightened to stabilise the segment.
3.Immediate postoperative period
After surgery, patients spend a short time in the recovery unit before returning to their room. Walking with support usually begins the same day or the next morning. Pain from the small incisions is generally well controlled, and the typical hospital stay is 2–3 nights depending on the case and number of levels treated.
Recovery after minimally invasive lumbar fusion
Recovery is gradual but generally faster than after open fusion. Light daily activities can usually be resumed within 1–2 weeks. Return to office work typically occurs between 3 and 6 weeks; physically demanding jobs require 2–4 months depending on the case.
Bony fusion takes several months to consolidate and is supported by a progressive rehabilitation programme: daily walking, core strengthening and gradual return to activity. The skin scars are small and discreet, which also helps the postoperative period.
Fever, worsening pain, wound drainage, new weakness or bowel/bladder changes warrant prompt medical review.
Risks and possible complications
Any surgery carries general risks such as infection, bleeding, deep vein thrombosis or anaesthesia-related issues. In MIS lumbar fusion, less muscle trauma usually means lower blood loss and lower wound infection rates than with an open approach.
Specific risks include screw misplacement, injury to a nerve root or dura (CSF leak), pseudarthrosis or non-union of the fusion, hardware loosening or breakage, and accelerated degeneration of adjacent levels over time. Intraoperative radiation from fluoroscopy is another factor and is minimised with careful technique or with navigation.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala