Facet joint blocks (cervical and lumbar)
Facet joint blocks are image-guided injections that deliver a local anaesthetic —often with a corticosteroid— inside or around the facet joint, one of the most common sources of mechanical neck and low-back pain. They serve two purposes: confirming that the pain originates from that joint and providing temporary relief when conservative treatment is not enough. In patients who respond well, a positive block is also the key criterion to indicate a longer-lasting facet radiofrequency rhizotomy.
What is a facet joint block?
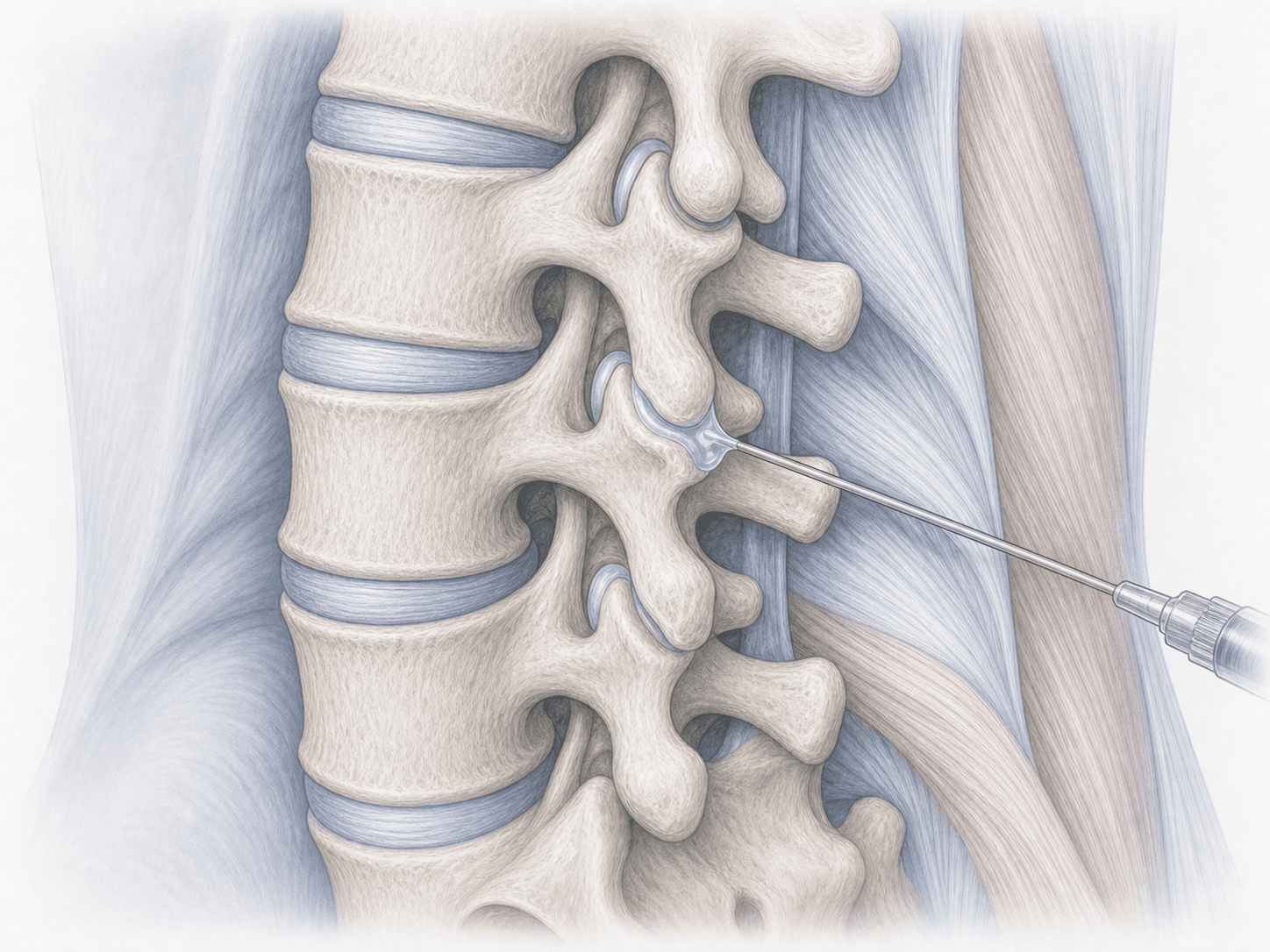
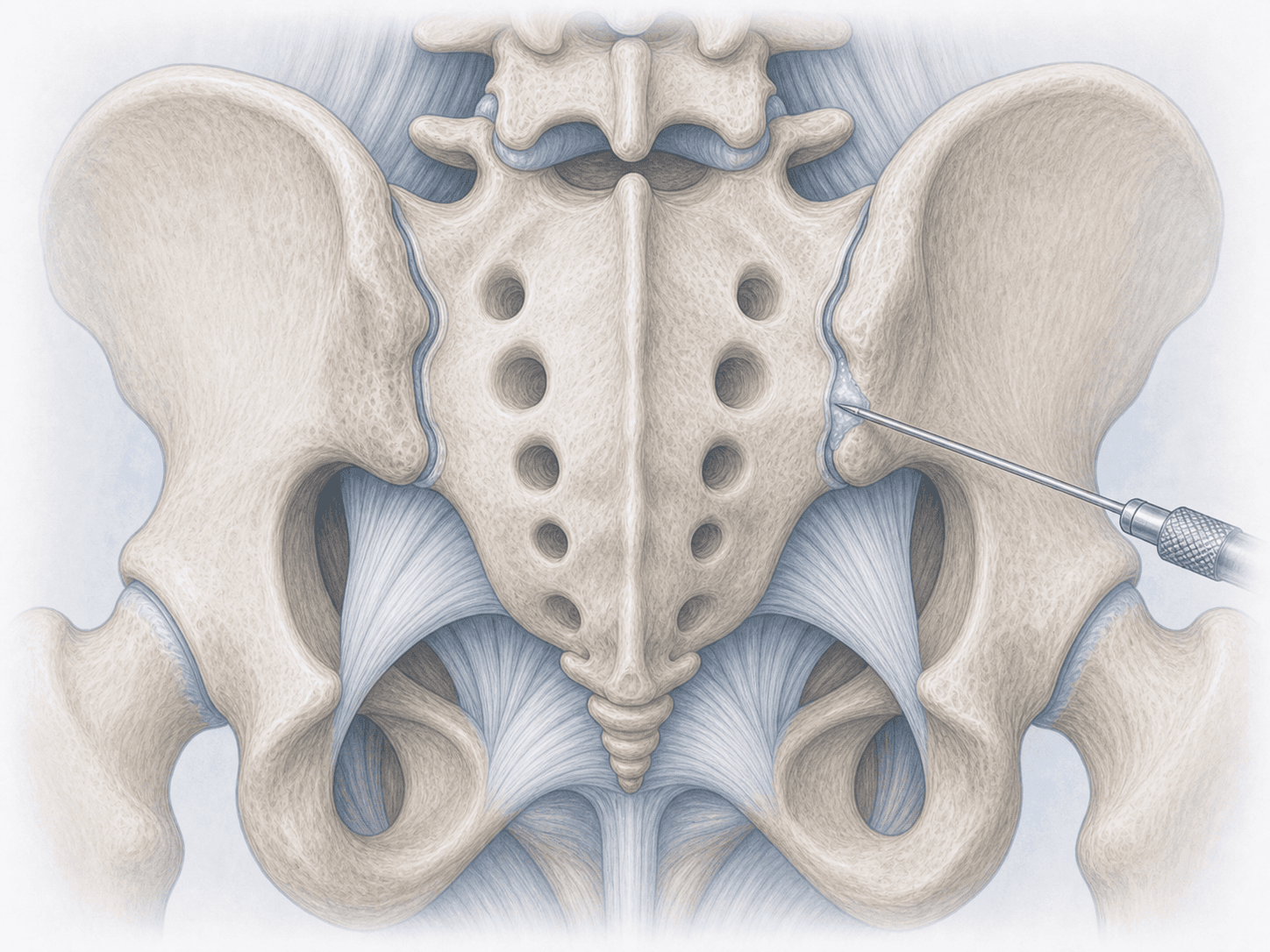
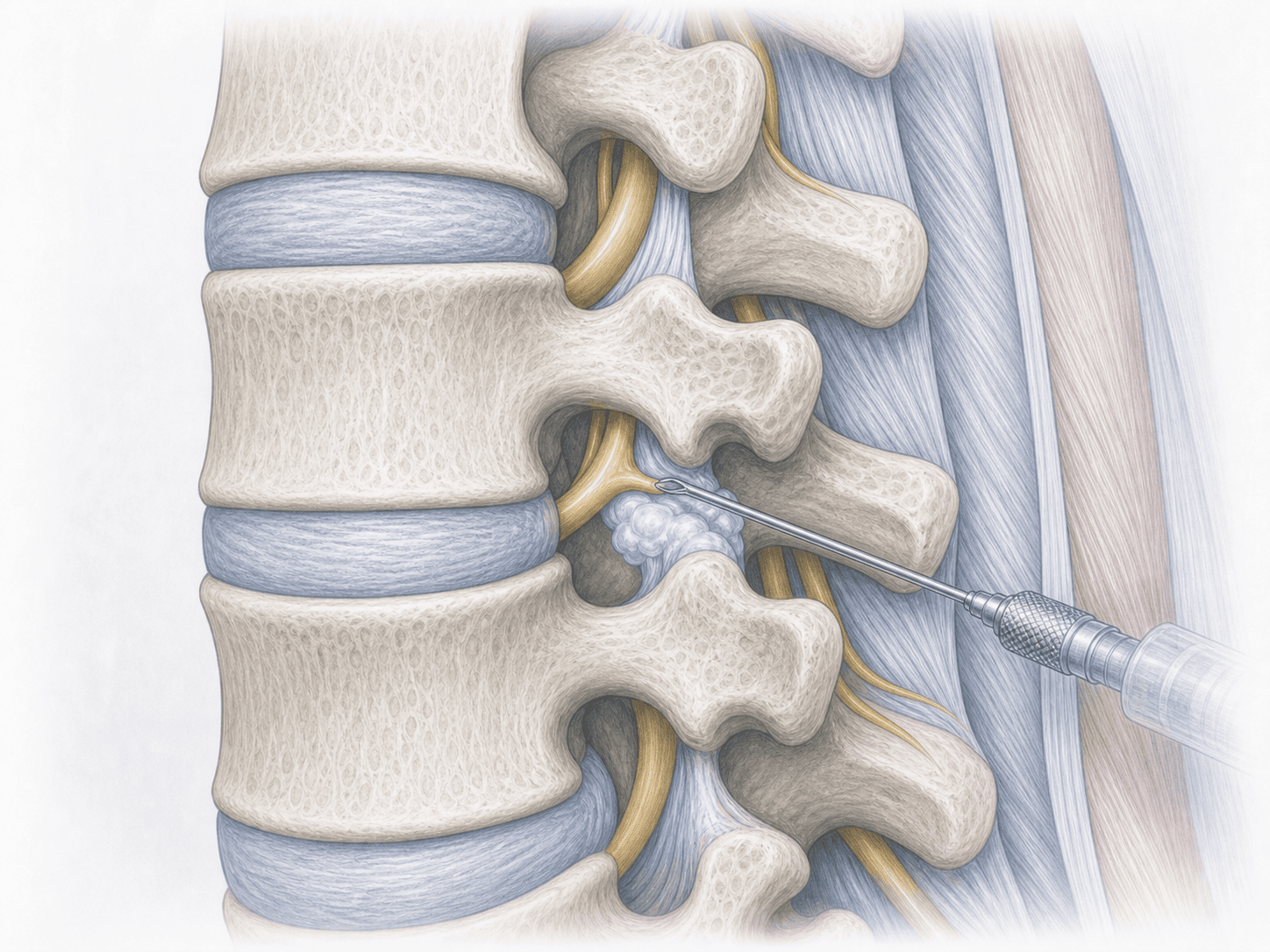
A facet joint block is an image-guided injection (fluoroscopy or ultrasound) in which a small amount of local anaesthetic, usually combined with a corticosteroid, is delivered into the facet joint or onto the medial branch nerve that supplies it. Facet joints are the small posterior joints of the spine that allow motion between vertebrae and often become painful when they are inflamed or degenerated.
The block has two roles: as a diagnostic test, it helps confirm that neck or low-back pain truly comes from the facet joint; as a treatment, it relieves pain for weeks or months thanks to the anti-inflammatory effect of the steroid. When initial relief is clear but short-lived, a facet radiofrequency rhizotomy is often indicated to achieve longer-lasting relief.
To find out whether a facet block is right for you, you can request an assessment with Dr. Ben Ghezala.
Symptoms that suggest facet-mediated pain
Facet-mediated pain has a recognisable pattern in clinical practice. Typical features include:
When is a facet block indicated?
How is a facet joint block performed?
1.Preparation before the block
Your history, examination and imaging are reviewed to identify the levels to be injected. Active infection, relevant allergies and anticoagulant therapy are checked and adjusted when needed. Strict fasting is usually not required, but specific instructions are provided for each case.
2.During the procedure
You lie face down and a small amount of local anaesthetic is applied to the skin. Under fluoroscopy (real-time X-ray) or ultrasound, a thin needle is advanced into the facet joint or onto the corresponding medial branch. A mixture of local anaesthetic and, in most cases, a depot corticosteroid is injected. Several levels can be treated in the same session, on one or both sides if needed. The procedure usually takes 15 to 30 minutes.
3.After the block
You are observed for 20 to 60 minutes after the injection. You are asked to record how much relief you feel during the first hours (anaesthetic effect) and over the following days (steroid effect), because this response guides the next step. Most patients walk home the same day, avoiding driving for the first few hours.
Recovery and outcome after a facet block
During the first hours the anaesthetic gives a fast answer about how much pain truly comes from the treated facets. A mild rebound at 24–48 hours is common before the steroid starts to act between day 3 and day 7.
Relief can last from several weeks up to a few months, depending on the degree of facet arthritis and the patient's activity. Use this window to resume physiotherapy, therapeutic exercise and postural correction.
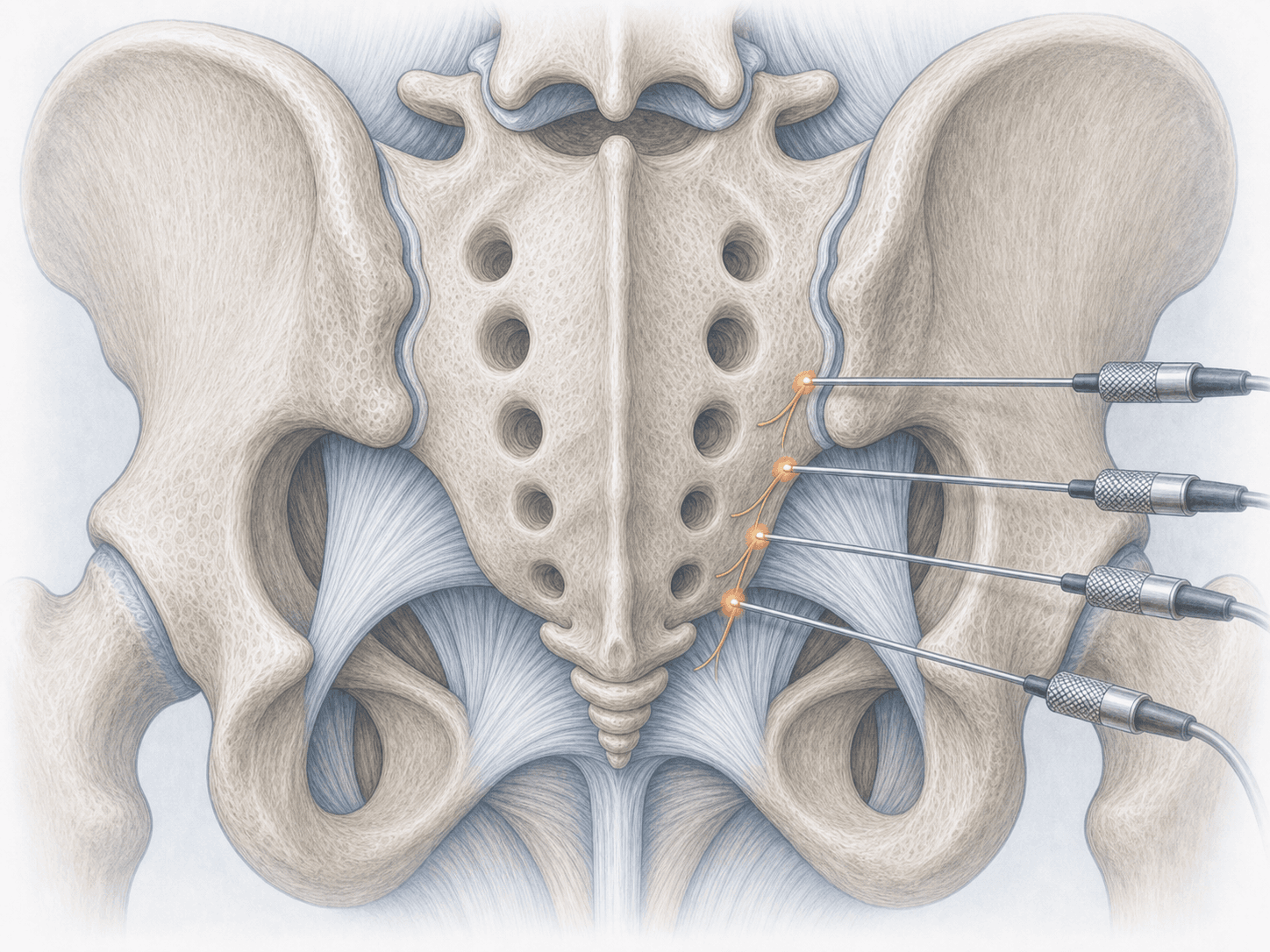
If the block clearly confirms a facet origin but the relief is short-lived, a facet radiofrequency rhizotomy is usually proposed to obtain longer-lasting benefit.
Risks and possible side effects
Image-guided facet joint blocks are very safe procedures, but they are not risk-free.
Possible effects include local discomfort or a temporary flare of pain at the injection site, a small bruise, a vasovagal reaction, mild elevation of blood sugar or blood pressure related to the corticosteroid and, less commonly, drug allergy or infection. In cervical procedures there is also a very low risk of vascular puncture, which is why image guidance is always used. Fever, any new neurological symptom or disproportionate pain should be reported promptly.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala