Craniocervical decompression for Chiari I
Craniocervical decompression is the reference operation for symptomatic Chiari I malformation, when the cerebellar tonsils descend through the foramen magnum and compress the brainstem or disturb cerebrospinal fluid flow. Many patients reach our clinic in Alicante or Benidorm after years of occipital cough headache, dizziness, tingling or a syringomyelia cyst recently seen on MRI. This guide explains honestly when we recommend surgery, what the technique involves and how recovery feels, so you can make a calm and fully informed decision.
What is craniocervical decompression for Chiari I?
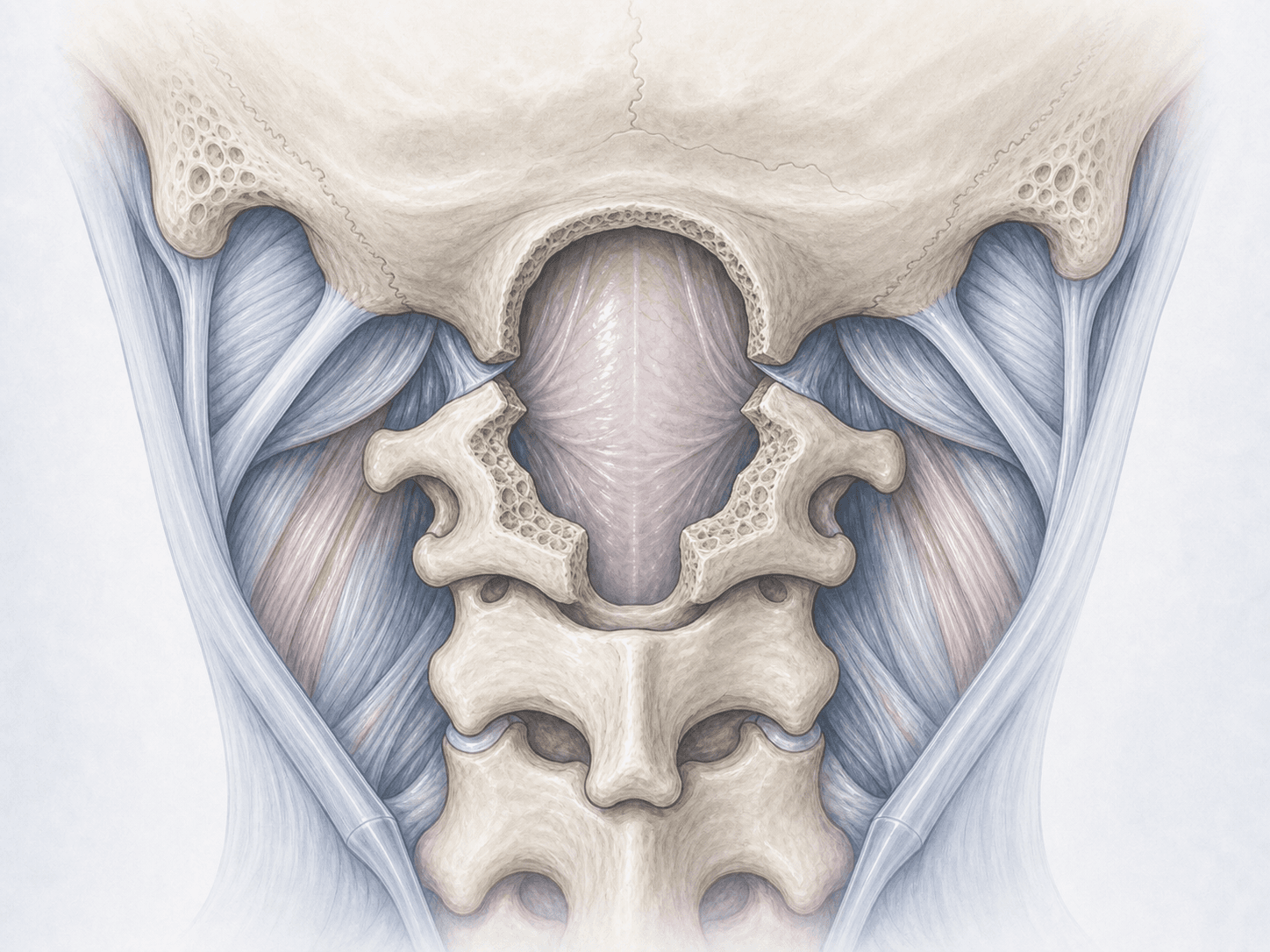
Craniocervical decompression is a surgical procedure that enlarges the space at the base of the skull and the upper neck so that descended cerebellar tonsils no longer compress the brainstem and cerebrospinal fluid can flow normally. A small suboccipital craniectomy is performed, usually together with a laminectomy of the posterior arch of C1.
In patients with neurological symptoms or associated syringomyelia, decompression is the only option that halts progression and may relieve the typical cough headache. When cervical spinal cord compression coexists, we assess whether to combine it with a cervical myelopathy decompression. To discuss your case, you can request an assessment with Dr. Ben Ghezala in Alicante or Benidorm.
Symptoms and warning signs
People with Chiari I who may benefit from surgery typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
We review the brain and cervical MRI, cerebrospinal fluid flow studies where available and a complete neurological examination. Blood tests, an electrocardiogram and an anaesthesia consultation are arranged. You will receive fasting instructions, medication adjustments and recommendations to optimise the procedure.
2.During the procedure
Surgery is performed under general anaesthesia with the patient prone and the head fixed. We make a midline vertical incision, remove a small bony fragment from the suboccipital region (craniectomy) and remove the posterior arch of C1 when needed. Under the microscope we decide whether to open the dura and perform a duraplasty with a graft to enlarge the cerebrospinal fluid space, weighing benefits and risks for each individual case.
3.Immediate postoperative period
You will spend a few hours in the recovery unit with close neurological monitoring before going up to the ward. We monitor pain, temperature and the surgical wound. Mobilisation usually starts within the first 24 hours. Hospital stay is typically 3 to 5 days, longer when a duraplasty has been performed.
Recovery after craniocervical decompression
Cough headache often improves significantly within the first weeks, while tingling or arm strength recover more gradually. It is wise to avoid strenuous effort, forced coughing and Valsalva manoeuvres during the first month.
Return to office work usually happens between 3 and 6 weeks, and physical tasks or sport are reintroduced gradually from the second or third month. When syringomyelia was present, we arrange follow-up MRIs at 3, 6 and 12 months to confirm its reduction. Fever, fluid leak from the wound, very severe headache or new neurological symptoms require prompt medical review.
Risks and possible complications
Any surgery carries general risks including infection, bleeding, thrombosis or anaesthesia-related complications.
Specific risks of craniocervical decompression include cerebrospinal fluid leak, pseudomeningocele, aseptic meningitis, persistent headache, cerebellar or brainstem injury (uncommon), craniocervical instability and the need for revision surgery if decompression proves insufficient or if a duraplasty develops a fistula. These risks are assessed individually and explained in detail during the consultation.
Frequently asked questions
Other related treatments



Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala