Lateral recess decompression
Lateral recess decompression is a lumbar microsurgical procedure designed to release the nerve root trapped in the subarticular space, a common cause of leg pain and unilateral neurogenic claudication. Many patients reach this option after months of persistent symptoms, weakness or walking limitation that has not improved enough with physiotherapy, medication or injections. This guide walks you through the procedure step by step —indications, technique, recovery and risks— so you can make a calm, well-informed decision.
What is lateral recess decompression?
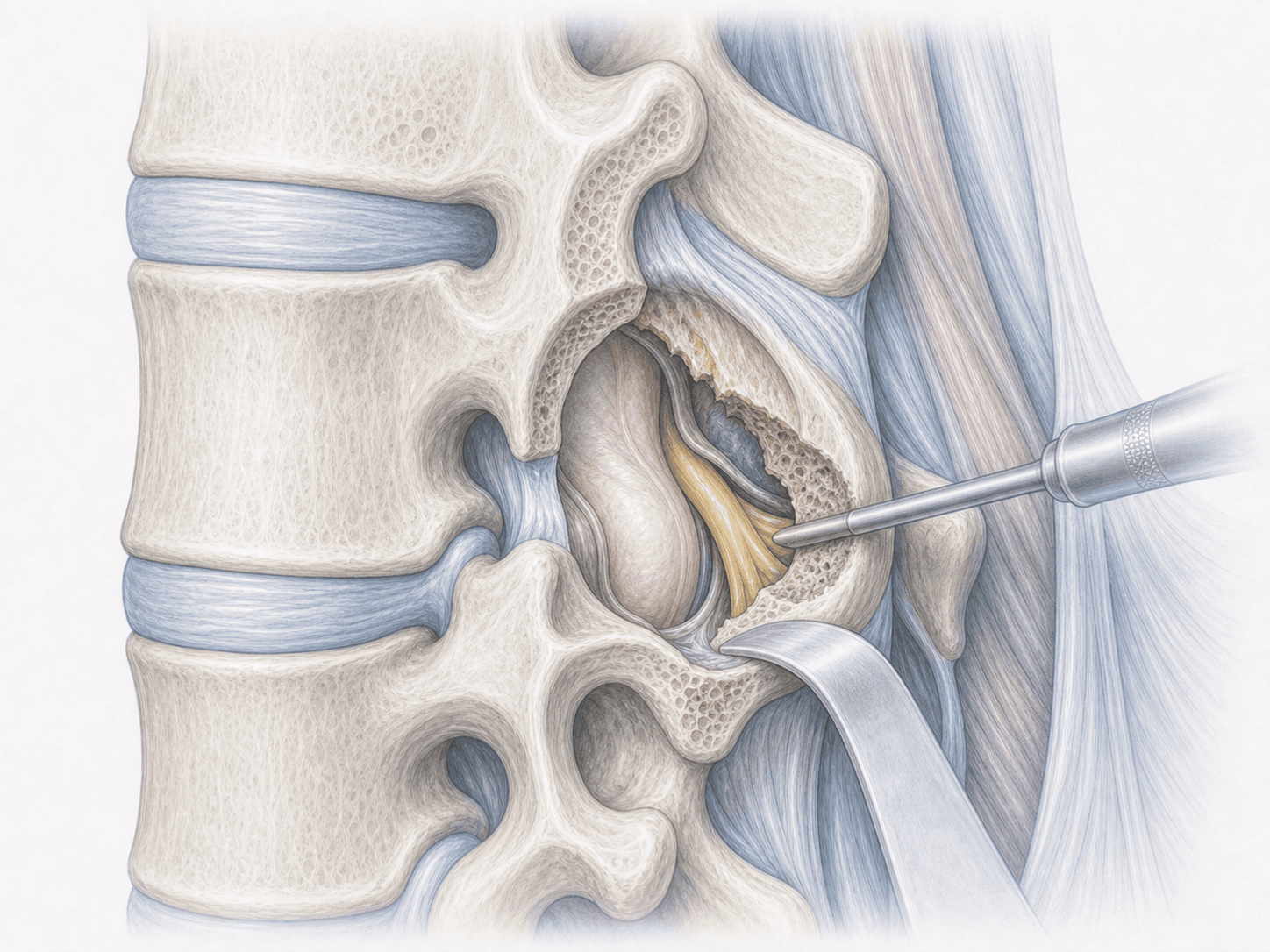
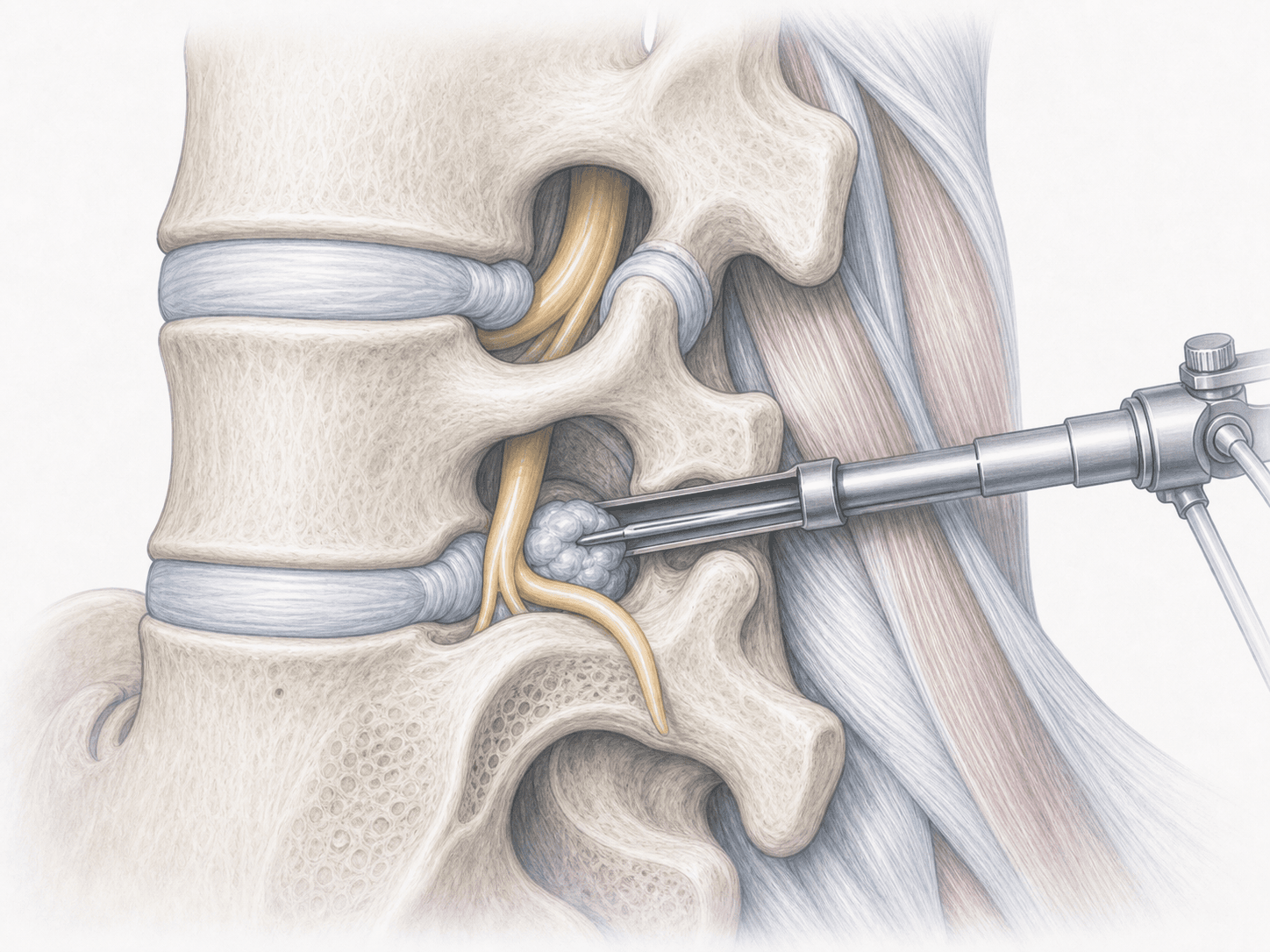
Lateral recess decompression is a lumbar microsurgical procedure aimed at releasing the nerve root trapped in the subarticular space, just before it exits through the foramen. The lateral recess is a narrow corridor bordered by the superior facet, the pedicle and the vertebral body; when it narrows due to facet hypertrophy, ligamentum flavum thickening or disc protrusion, it compresses the traversing root.
Our preferred approach is microsurgical undercutting: we work under the microscope to remove the medial and inferior portion of the superior facet without sacrificing the entire joint. This decompresses the root while preserving segmental stability and avoids fusion when it is not needed.
It is a more selective alternative to a classic lumbar laminotomy and is particularly useful in patients with unilateral radicular pain or neurogenic claudication caused by focal lateral recess stenosis. If you would like to review your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients with lateral recess stenosis usually describe a fairly characteristic radicular pattern:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
We review the MRI together and, if needed, a CT scan to assess the bony anatomy of the facet. We pinpoint the affected root and the level to be treated. You receive fasting instructions, guidance on adjusting anticoagulants and anti-inflammatories, and we address any questions about anaesthesia and recovery.
2.During the procedure
The procedure is performed under general anaesthesia, in prone position, with fluoroscopic guidance to confirm the level. We use a small posterior approach centred on the affected segment and work under the operating microscope for better visualisation and precision.
We perform a limited laminotomy and, using the undercutting technique, drill away the medial and inferior portion of the superior facet and remove the hypertrophied ligamentum flavum. This opens the lateral recess and frees the root, which we confirm is mobile and tension-free. If a disc fragment is contributing, it is removed in the same step. Most of the facet joint is preserved, maintaining segmental stability.
3.Immediate postoperative period
After a short time in the recovery area, you return to your room. Mobilisation usually begins the same day or the following morning with nursing support. Pain is controlled with a tailored analgesic plan and we monitor your neurological status. Hospital stay is typically 24 to 48 hours depending on progress.
Recovery after lateral recess decompression
Lateral recess decompression usually relieves leg pain within the first days, though local wound discomfort and some lumbar soreness may linger for a few weeks. We recommend progressive walking from the start and avoiding prolonged bed rest.
Office work is typically resumed between 2 and 4 weeks. Jobs involving physical effort or lifting require more time, usually 6 to 8 weeks, with a gradual return. Rehabilitation, when indicated, helps restore strength and correct postural habits. Fever, wound discharge, sudden worsening of pain or new neurological deficits should prompt immediate contact with us.
Risks and possible complications
Like any surgery, it carries general risks: wound infection, bleeding, anaesthesia-related complications or venous thrombosis.
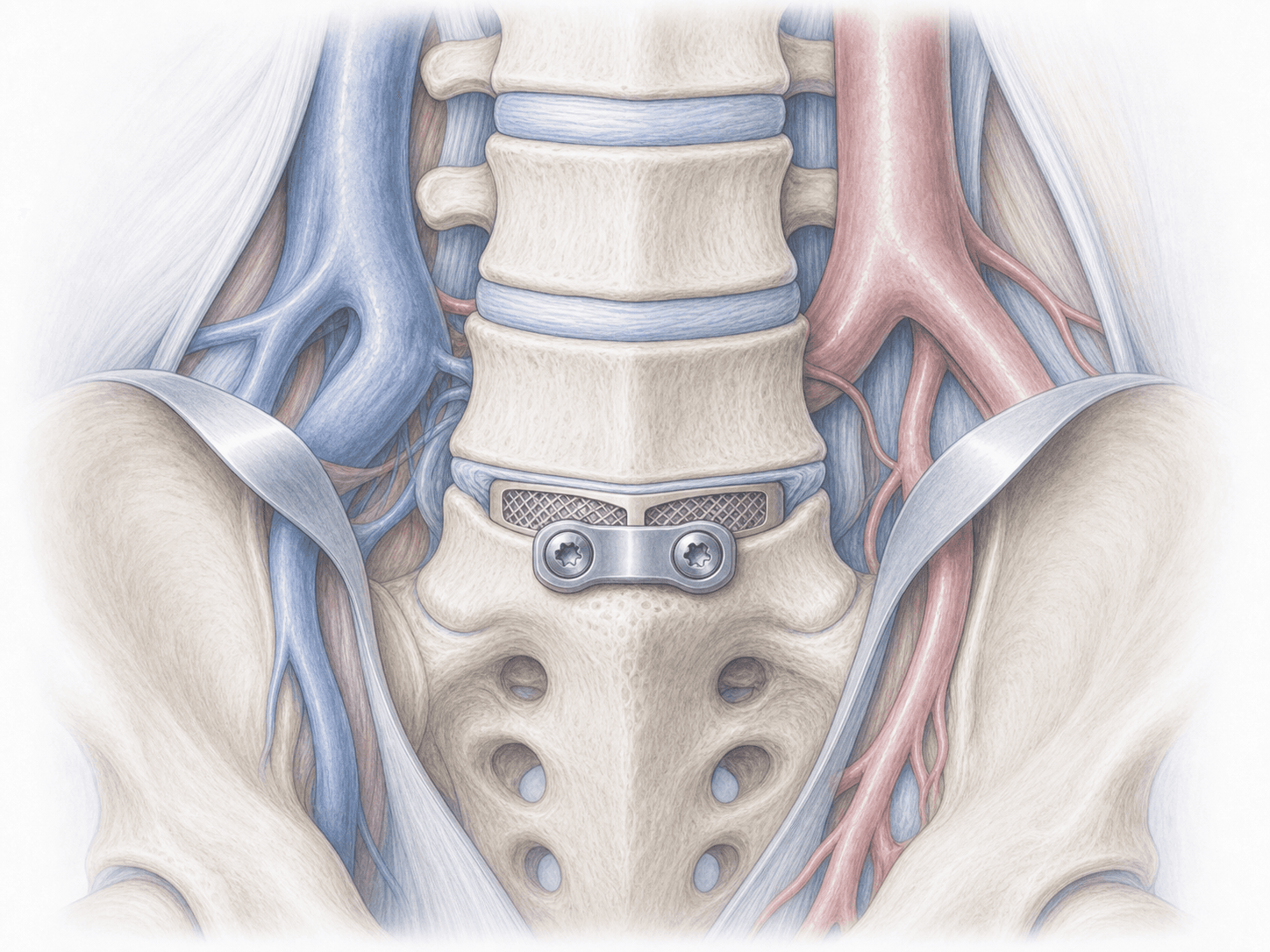
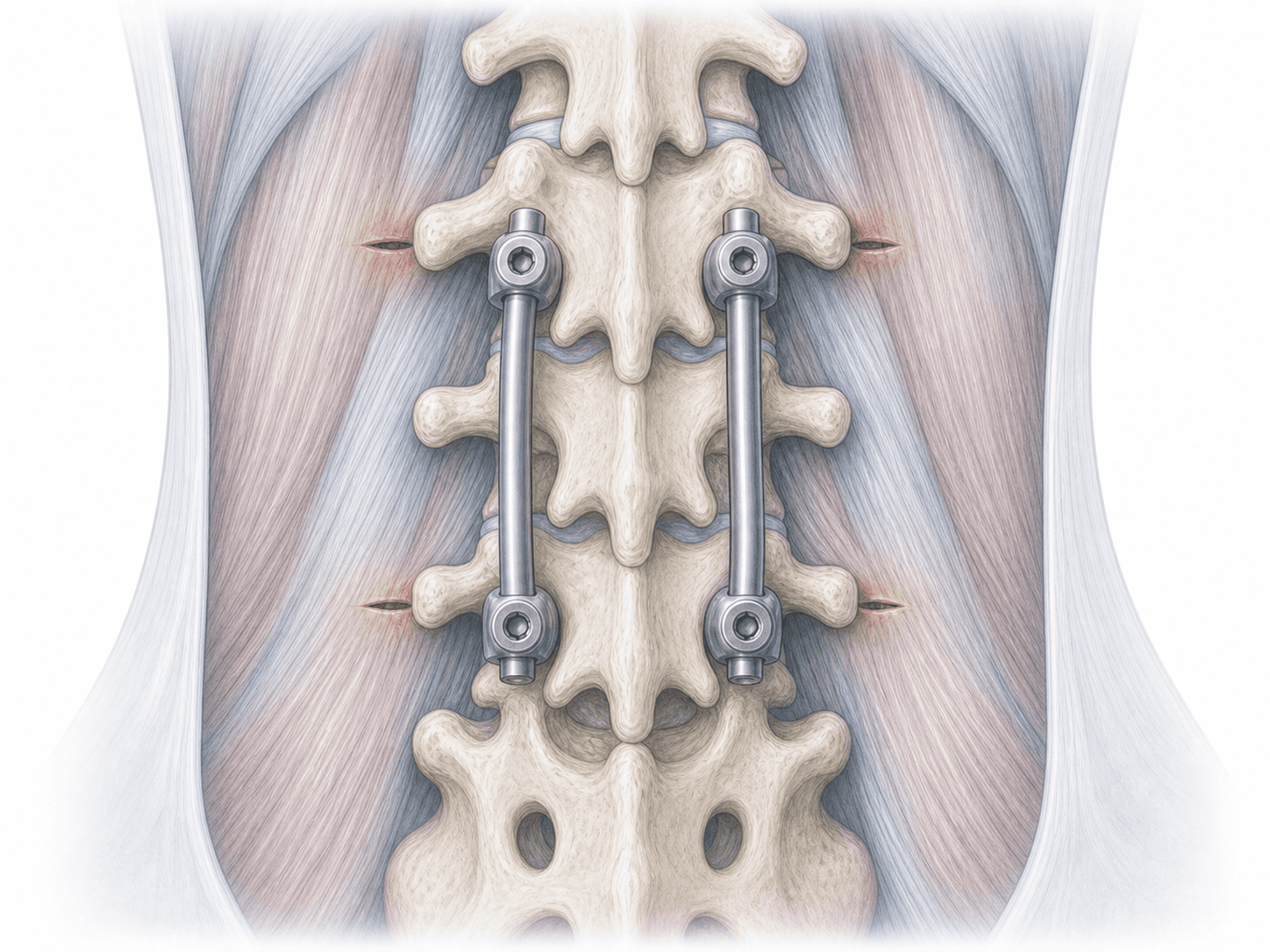
Specific risks include dural tear with cerebrospinal fluid leak, nerve root injury with sensory or motor deficit, recurrence of pain due to new stenosis or disc herniation, and very rarely postoperative instability if more bone than planned needed to be removed; in such cases a secondary fusion might be considered. Each case is assessed individually to minimise these risks.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala