Thoracic intraspinal tumour surgery
Thoracic intraspinal tumour surgery is the microsurgical resection of intradural lesions (schwannomas, meningiomas, ependymomas or other) located within the spinal canal at the thoracic level. This segment is particularly delicate: the thoracic canal is narrow, the spinal cord tolerates manipulation poorly and its blood supply depends largely on the artery of Adamkiewicz. The surgical decision and technique must therefore be highly precise. This guide explains when this surgery is indicated, how it is performed and what recovery to expect, with a realistic approach to support an informed decision.
What is thoracic intraspinal tumour surgery?
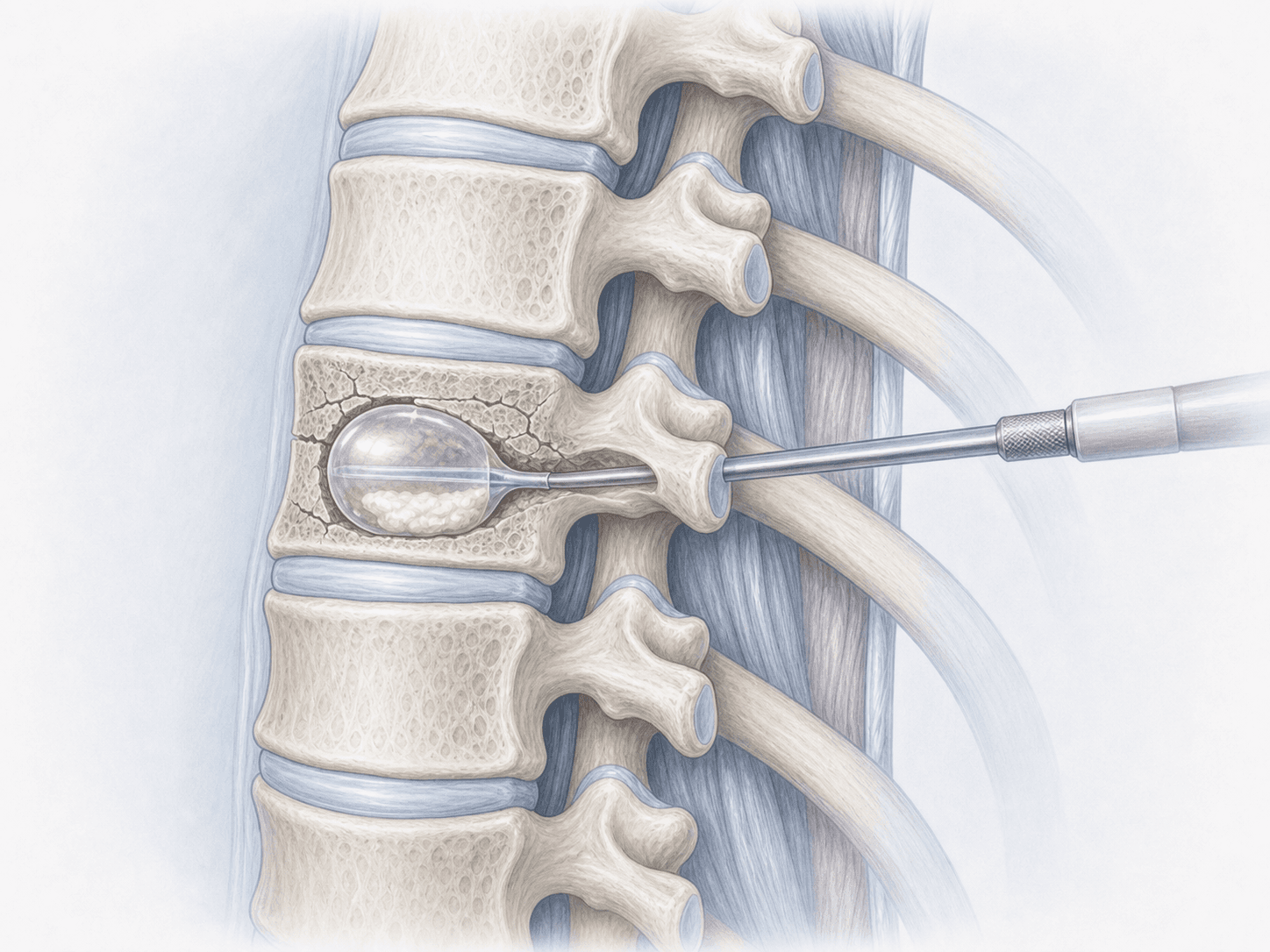
Thoracic intraspinal tumour surgery is a microsurgical procedure aimed at removing lesions located within the spinal canal at the thoracic level, either outside the spinal cord (extramedullary, such as schwannomas or meningiomas) or within it (intramedullary, such as ependymomas or astrocytomas).
Compared with general intraspinal tumour surgery, the thoracic approach requires specific considerations: a narrow spinal canal, a spinal cord that tolerates retraction poorly and a blood supply that depends on the artery of Adamkiewicz. Intraoperative neuromonitoring (motor and somatosensory evoked potentials) and meticulous microsurgical technique are therefore essential. To discuss your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Thoracic intraspinal tumours can present insidiously and progressively. Medical assessment is advisable in the following situations:
When is this surgery indicated?
How is the procedure performed?
1.Preoperative preparation
A detailed clinical assessment is performed, with review of the contrast-enhanced MRI and, if needed, additional studies (CT, MR angiography) to localise the artery of Adamkiewicz and plan the approach. Realistic goals and the specific risks of the thoracic level are discussed, and medication is adjusted. Fasting instructions and antibiotic and thromboembolic prophylaxis are confirmed.
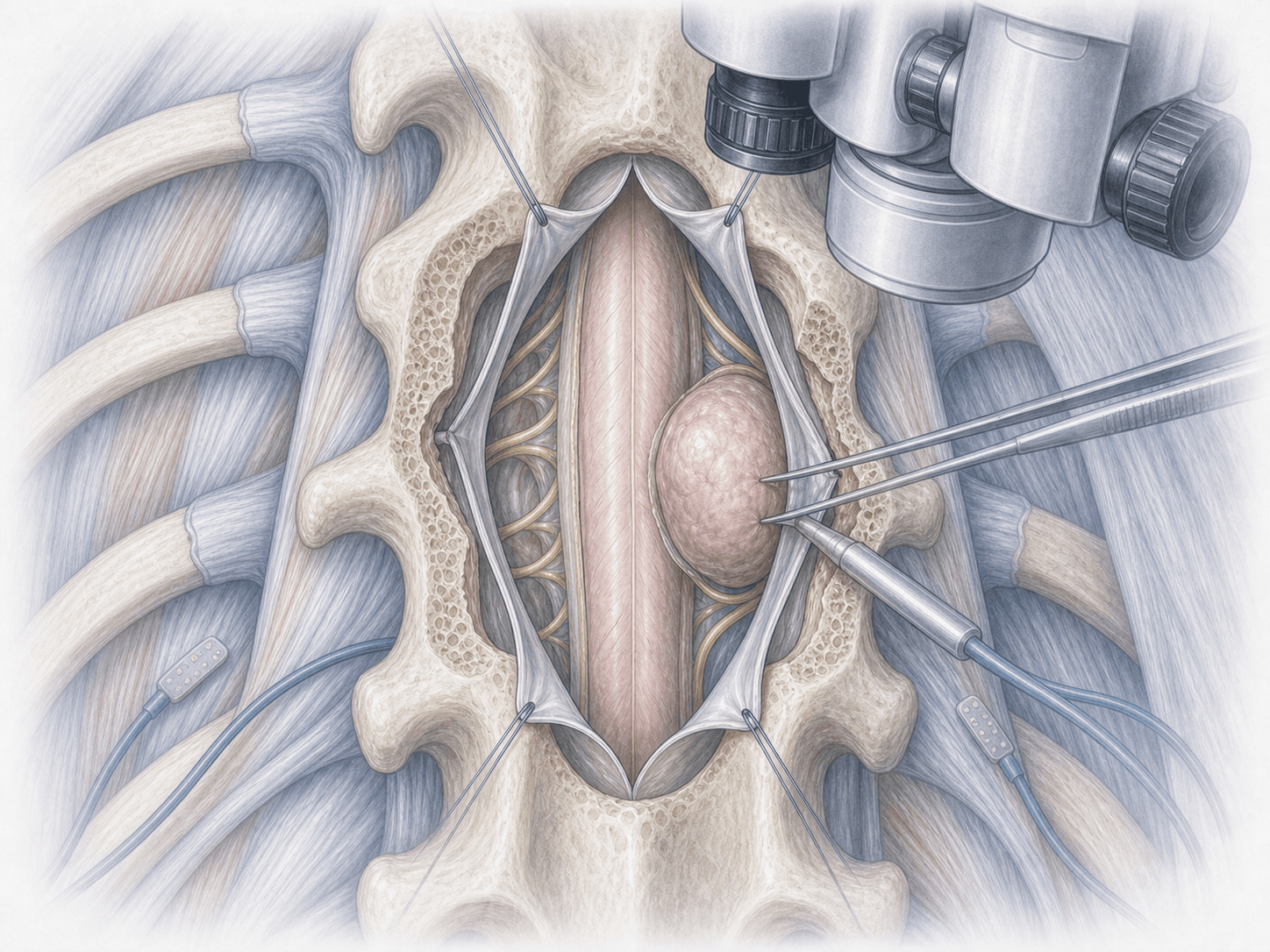
2.During the procedure
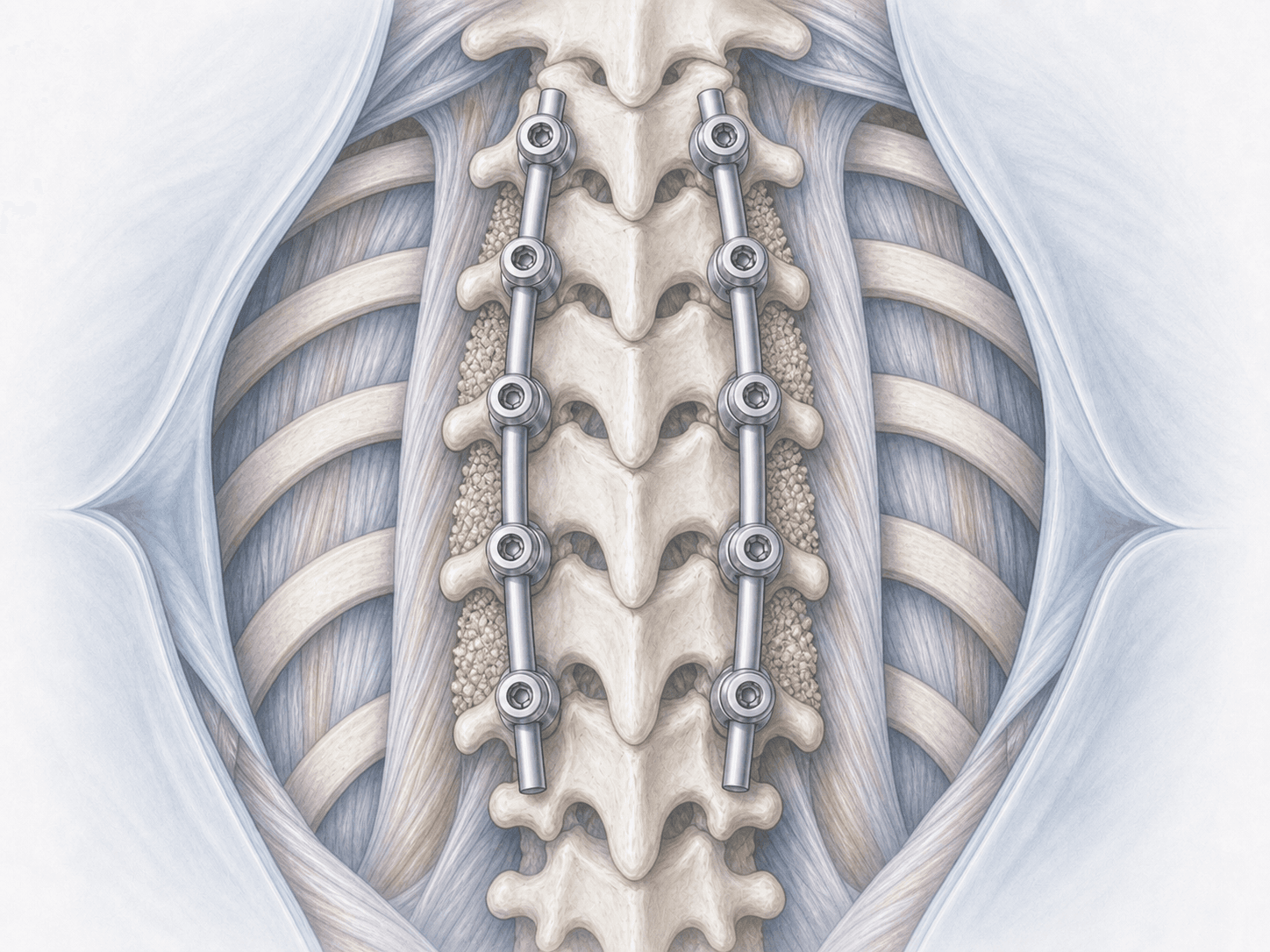
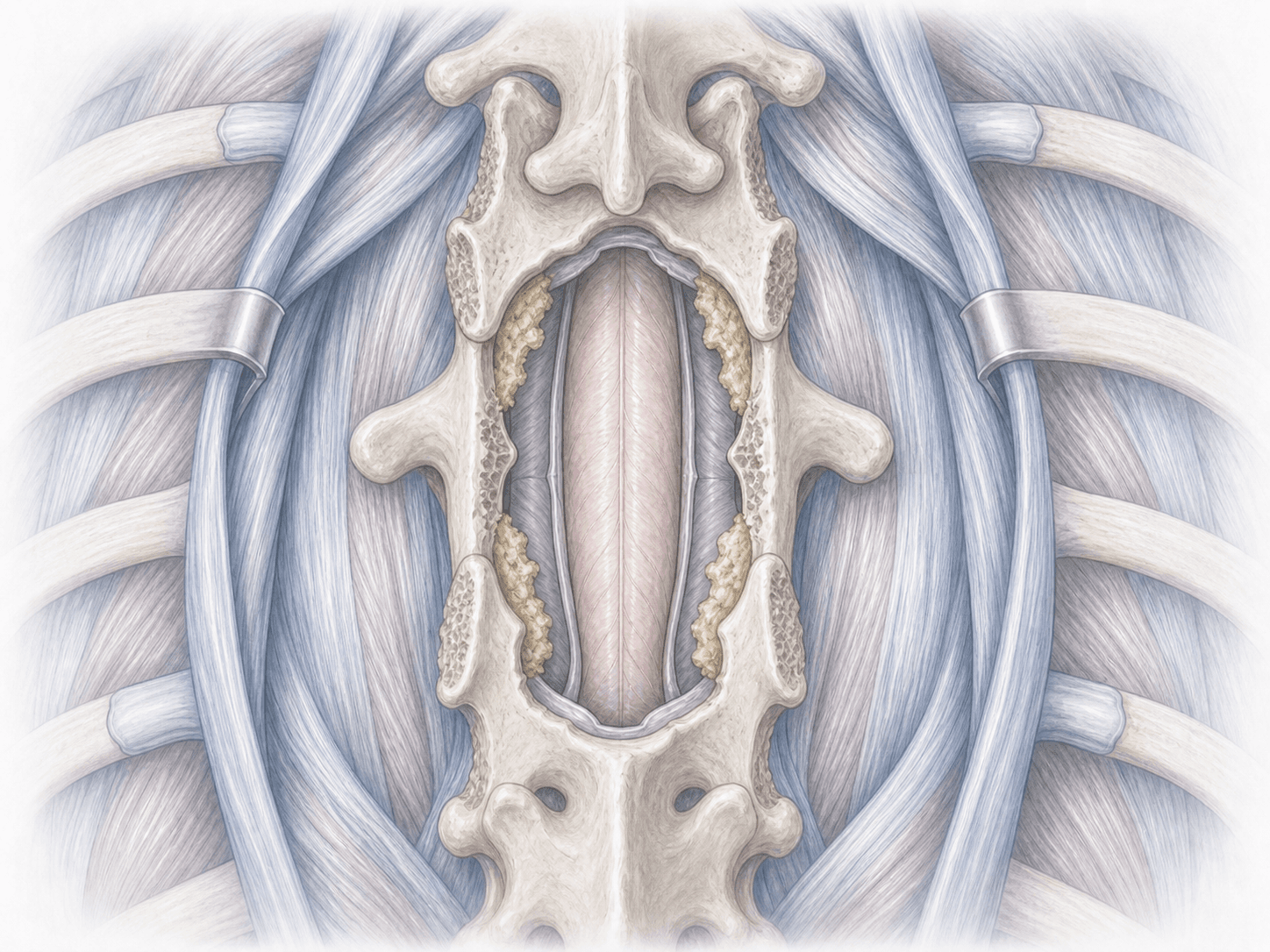
Surgery is performed under general anaesthesia with continuous intraoperative neuromonitoring (motor and somatosensory evoked potentials). A posterior approach with single- or multilevel laminectomy is typically used to access the spinal canal. Under the surgical microscope, the dura is opened and the tumour identified. Resection is microsurgical, carefully separating the tumour from the spinal cord and nerve roots; intramedullary lesions are approached through a minimal myelotomy, always guided by neuromonitoring. After resection, the dura is closed in a watertight fashion and, depending on the case, instrumentation may be added if segmental stability is compromised.
3.Immediate postoperative period
After surgery, patients spend several hours in recovery or ICU for close neurological monitoring. Pain is controlled, relative bed rest is maintained for the first 24–48 hours to support dural healing and early physiotherapy with progressive mobilisation is started. Hospital stay is usually 4–7 days, depending on clinical progress and intraoperative neuromonitoring findings.
Recovery after thoracic intraspinal tumour surgery
Recovery is gradual and depends on tumour type, its location within or outside the cord and the preoperative neurological status. The first weeks focus on protecting dural healing and retraining gait with adapted physiotherapy.
Many patients with extramedullary lesions (schwannomas, meningiomas) progressively regain strength and sensation over the first 3–6 months. With intramedullary lesions, improvement may be slower and sometimes partial, as the main goal is to halt deterioration and preserve function. Heavy lifting, driving and returning to work should wait for medical clearance. Fever, cerebrospinal fluid leak, sudden pain or new neurological symptoms warrant immediate review.
Risks and possible complications
All surgery carries general risks such as infection, bleeding, thrombosis and anaesthesia-related complications.
The specific risks of thoracic intraspinal surgery are particularly relevant due to the vulnerability of the spinal cord at this level: postoperative neurological deficit (weakness, sensory or sphincter changes) from spinal cord or vascular injury (including the artery of Adamkiewicz), cerebrospinal fluid leak, pseudomeningocele, segmental instability after multilevel laminectomy, tumour recurrence or the need for adjuvant oncological treatment. Intraoperative neuromonitoring and individualised planning reduce these risks but do not eliminate them entirely.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala