Thoracic foraminotomy
Thoracic foraminotomy is considered for patients with back pain that radiates in a band around the chest or abdomen, often described as burning, pressure or cramping along the path of an intercostal nerve. When medication, physiotherapy or nerve blocks no longer provide lasting relief and imaging shows narrowing of the thoracic foramen or a lateral foraminal disc herniation, this surgery opens that channel and frees the nerve through a posterolateral approach, preserving segment stability whenever possible. The goal is to relieve thoracic radicular pain without the need for fusion when feasible, with indication always personalised based on symptoms and imaging.
What is a thoracic foraminotomy?
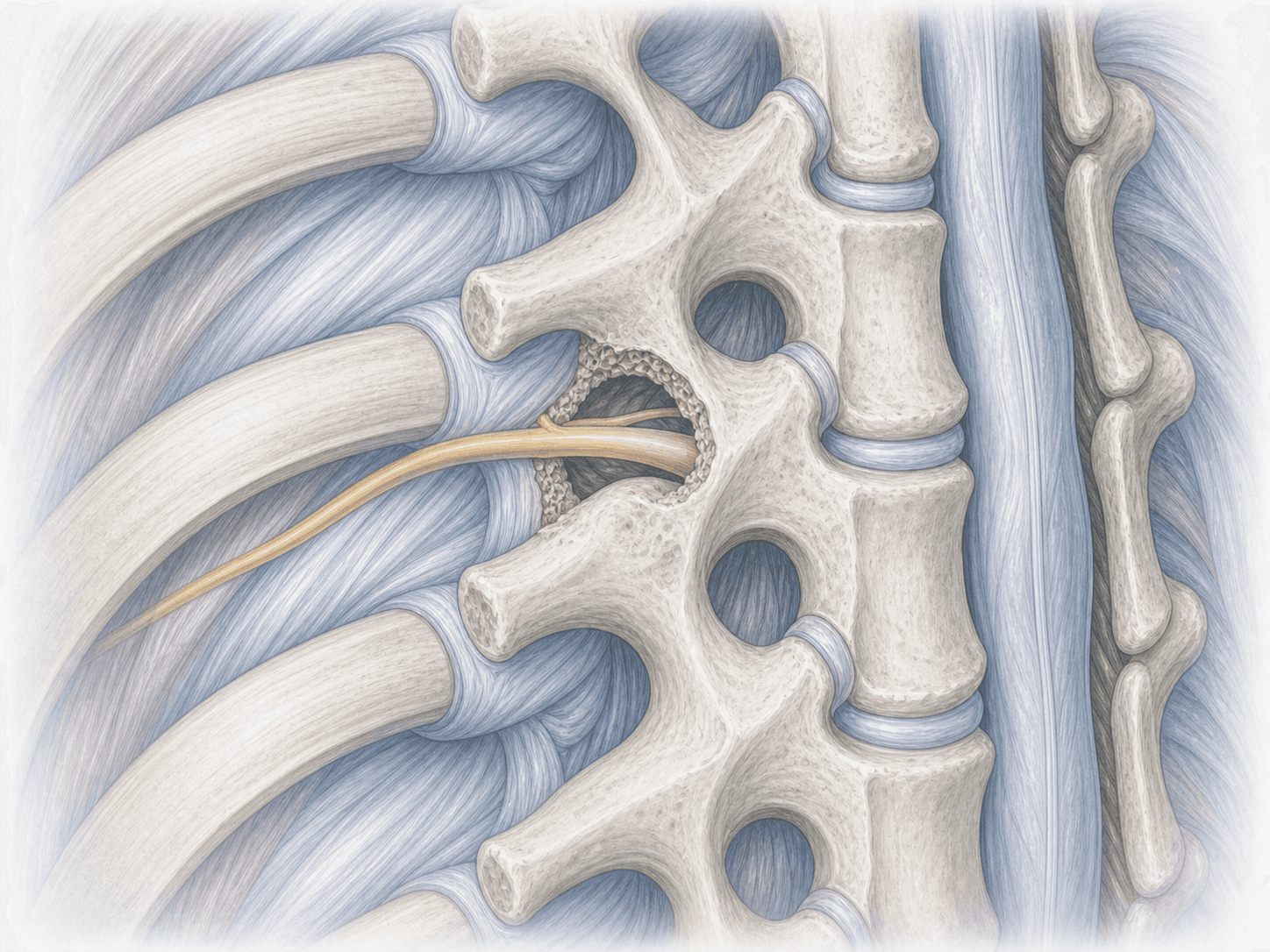
Thoracic foraminotomy is a focused surgery that widens the foramen through which a nerve root exits between two thoracic vertebrae. When that channel narrows due to facet arthritis, joint hypertrophy or a lateral foraminal disc herniation, the nerve becomes compressed and causes band-like pain around the chest or abdomen, following the path of the corresponding intercostal nerve.
Unlike a cervical foraminotomy, which is approached from the front or the back of the neck, in the thoracic spine we usually work from behind, using a posterolateral transpedicular approach or a limited costotransversectomy. This lets us reach the foramen without manipulating the spinal cord and, in most cases, without the need to fuse the segment.
It is an anatomically demanding procedure because the space is small and the thoracic cord is especially sensitive. That is why we only consider it when the diagnosis is clear and the radicular pain is genuinely limiting your life. To discuss your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from a thoracic foraminotomy typically describe:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
Includes a detailed clinical assessment, review of MRI and CT to pinpoint the exact level, and planning of the approach (transpedicular or limited costotransversectomy). Fasting rules, medication adjustments, antibiotic and thrombosis prophylaxis are explained, and any questions are addressed before admission.
2.During the procedure
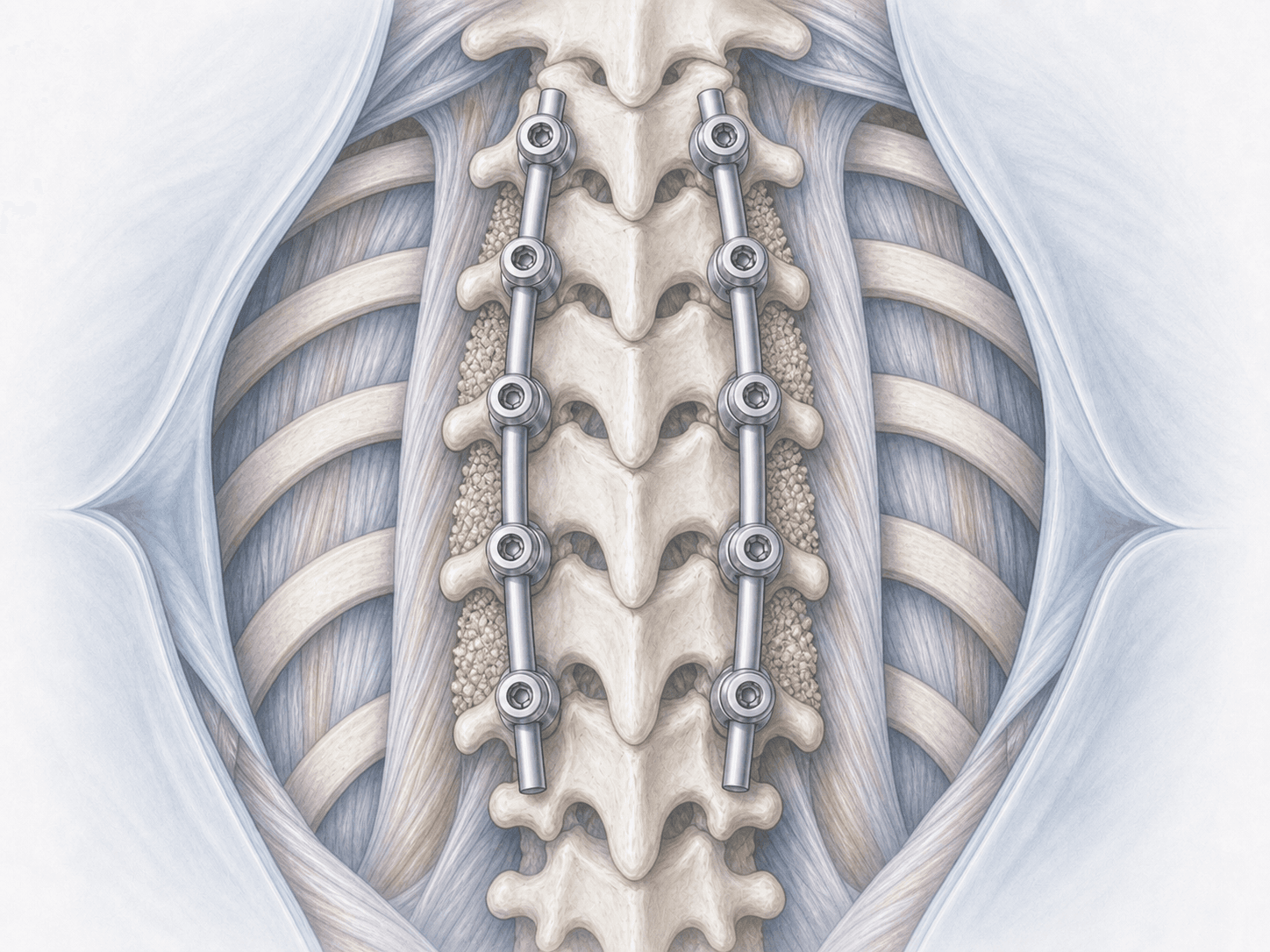
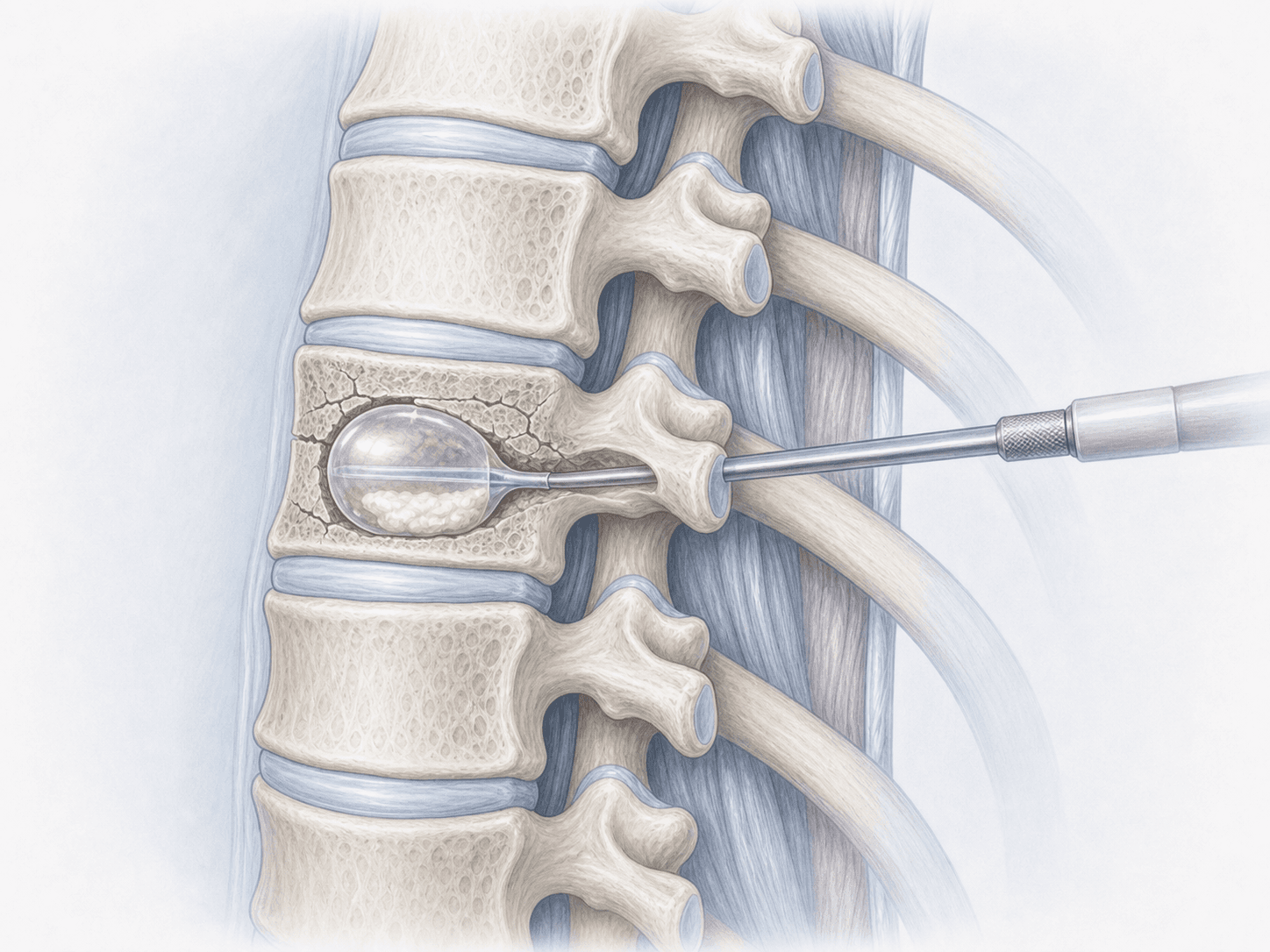
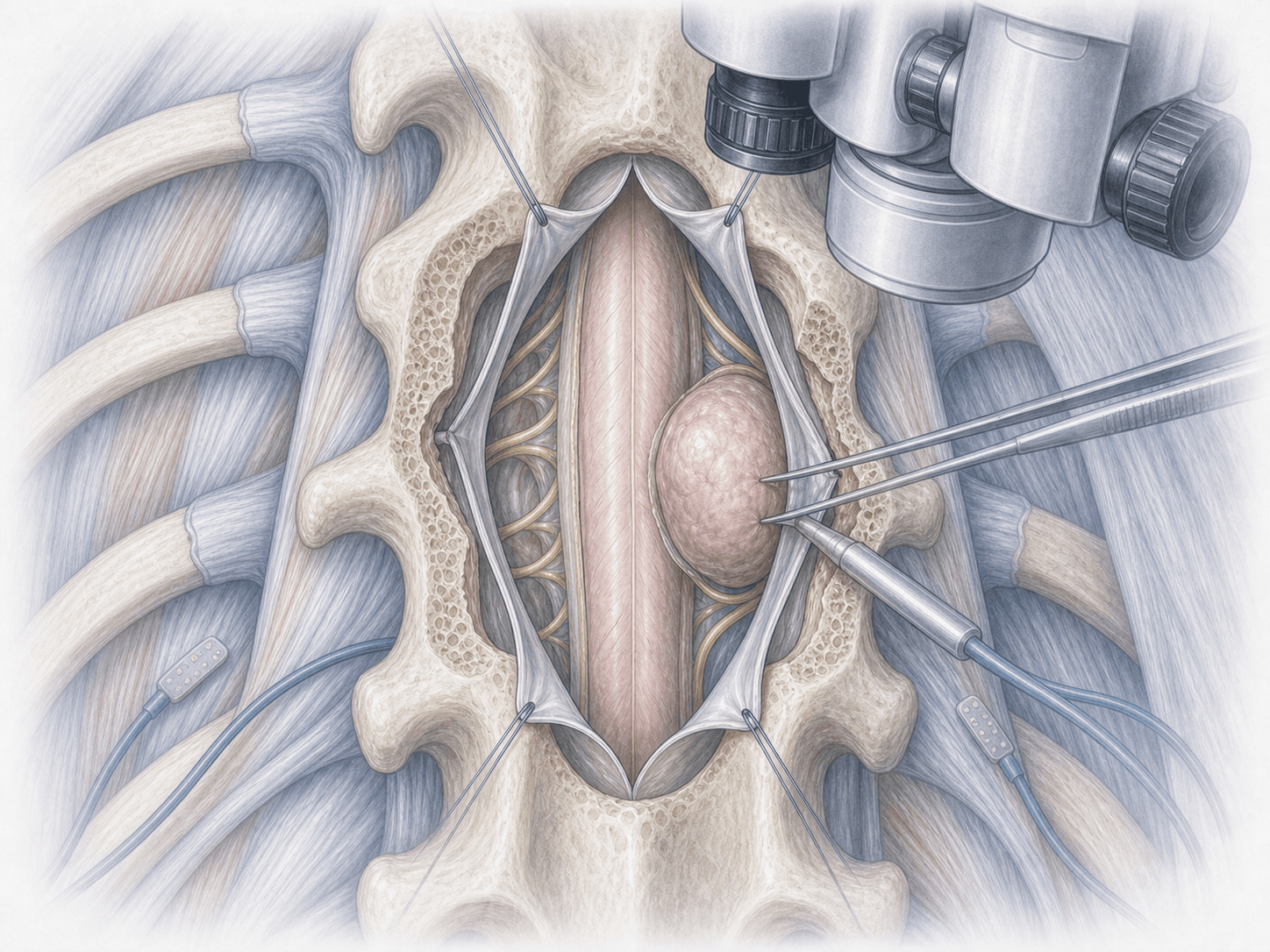
Under general anaesthesia and with the patient prone, we confirm the correct level with fluoroscopy and, when needed, with navigation. Through a small posterior incision we reach the foramen via a posterolateral route, carefully drilling part of the facet, the pedicle or the rib base depending on the case. We release the compressed intercostal nerve root and, if present, remove the foraminal disc fragment. We confirm decompression and close in layers. Most cases do not require fusion.
3.Immediate postoperative period
You spend a short time in recovery before returning to your room. Pain is controlled, leg neurological function and breathing mechanics are monitored, and gentle mobilisation begins within the first hours. Hospital stay is typically 24–72 hours depending on clinical progress.
Recovery after thoracic foraminotomy
Recovery is gradual. Light daily activities can usually be resumed within a few days, and office work between 3 and 5 weeks depending on progress. Physical jobs or those involving chest load require more time.
The band-like pain typically improves in the first few weeks, though the neuropathic component can take longer to settle, especially if the nerve had been compressed for a long time. Gentle respiratory physiotherapy, postural control and avoiding heavy loads and sudden rotations early on support a safe recovery. Fever, disproportionate pain, new leg weakness or bowel or bladder symptoms warrant prompt medical review.
Risks and possible complications
All surgery carries general risks such as infection, bleeding, thrombosis or anaesthesia-related complications.
Specific risks of thoracic foraminotomy include injury to the intercostal nerve root or spinal cord (uncommon), persistence or recurrence of neuropathic pain, pleural injury with pneumothorax when working very laterally, cerebrospinal fluid leak or, in selected cases, segmental instability that may later require fusion. These risks are assessed individually for each patient and discussed during informed consent.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala