ALIF — Anterior lumbar interbody fusion
Anterior lumbar interbody fusion (ALIF) is a surgical option for discogenic low back pain, instability or advanced degeneration when other treatments have not delivered lasting relief. The approach is performed through the front of the abdomen, which makes it possible to place a larger interbody cage, restore disc height and recover physiological lordosis at the treated level. Many patients consider this technique after years of low back pain that limits their daily life, work or sleep, despite physiotherapy, medication and injections. In this guide we explain, in plain language, when ALIF is indicated, how we work with a vascular surgeon as a team, what to expect during surgery and recovery and which specific risks we must discuss before making a decision.
What is ALIF (anterior lumbar interbody fusion)?
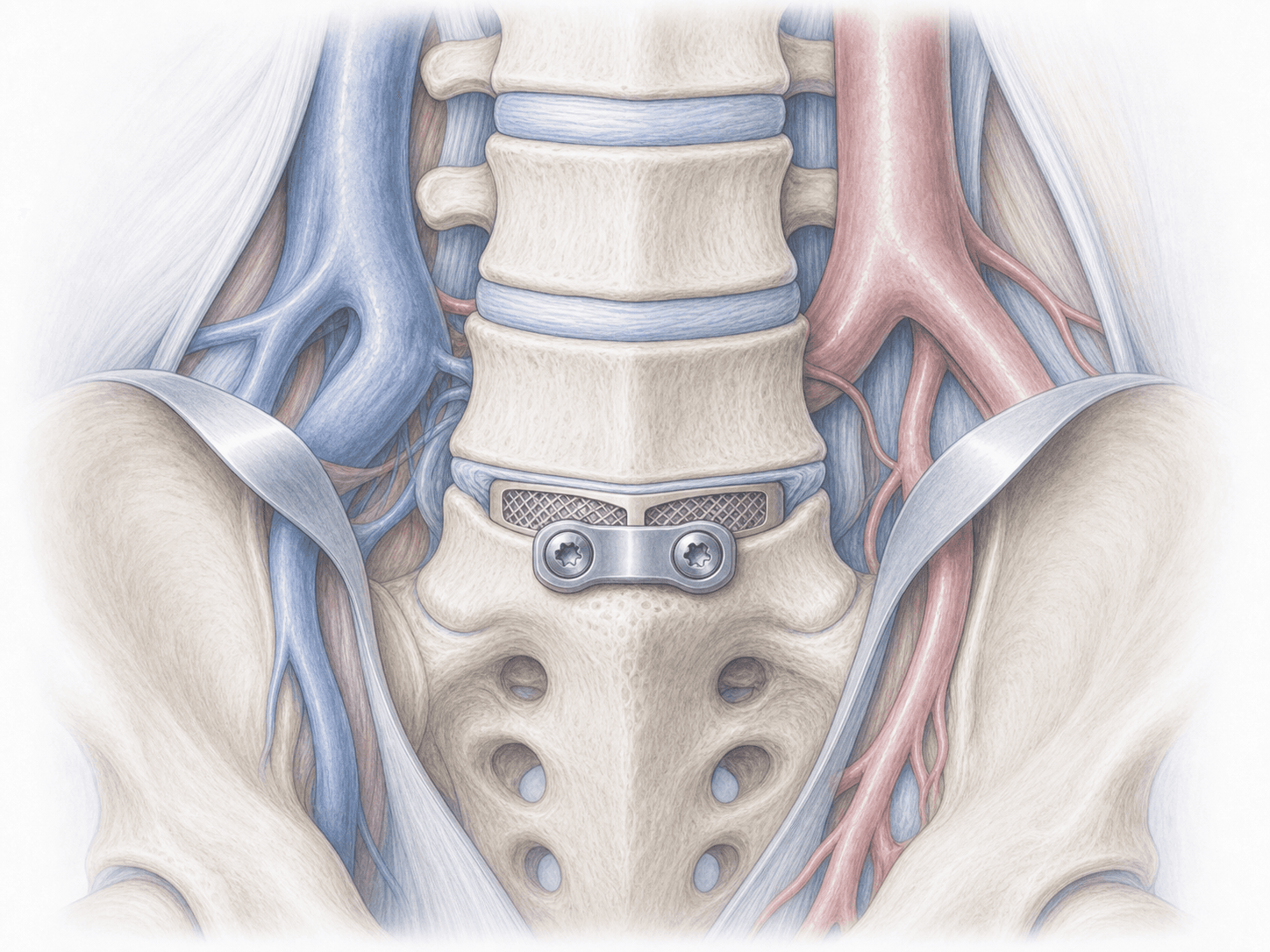
ALIF is a lumbar fusion procedure in which the degenerated disc is removed and replaced with an interbody cage through an anterior approach via the front of the abdomen, in collaboration with a vascular surgeon who carefully retracts the great vessels and the peritoneum. This access allows a larger implant than posterior or transforaminal techniques, helping to restore disc height, recover lordosis and indirectly decompress the foramen.
Compared with other lumbar fusions such as TLIF, PLIF or lateral and oblique fusions XLIF/LLIF/OLIF, the anterior route offers a wide bony contact surface and a more effective sagittal correction, particularly at L5-S1, where the lateral approach is more difficult. In exchange, it requires careful vascular planning and a multidisciplinary team. To assess whether ALIF is the best option for your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from ALIF typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
We confirm the indication with MRI, dynamic radiographs and, when needed, a CT angiogram or vascular study to plan the approach with the vascular surgeon. We review the procedure, specific risks and alternatives with you, adjust medication (anticoagulants, antiplatelets) and provide fasting and preparation instructions.
2.During the procedure
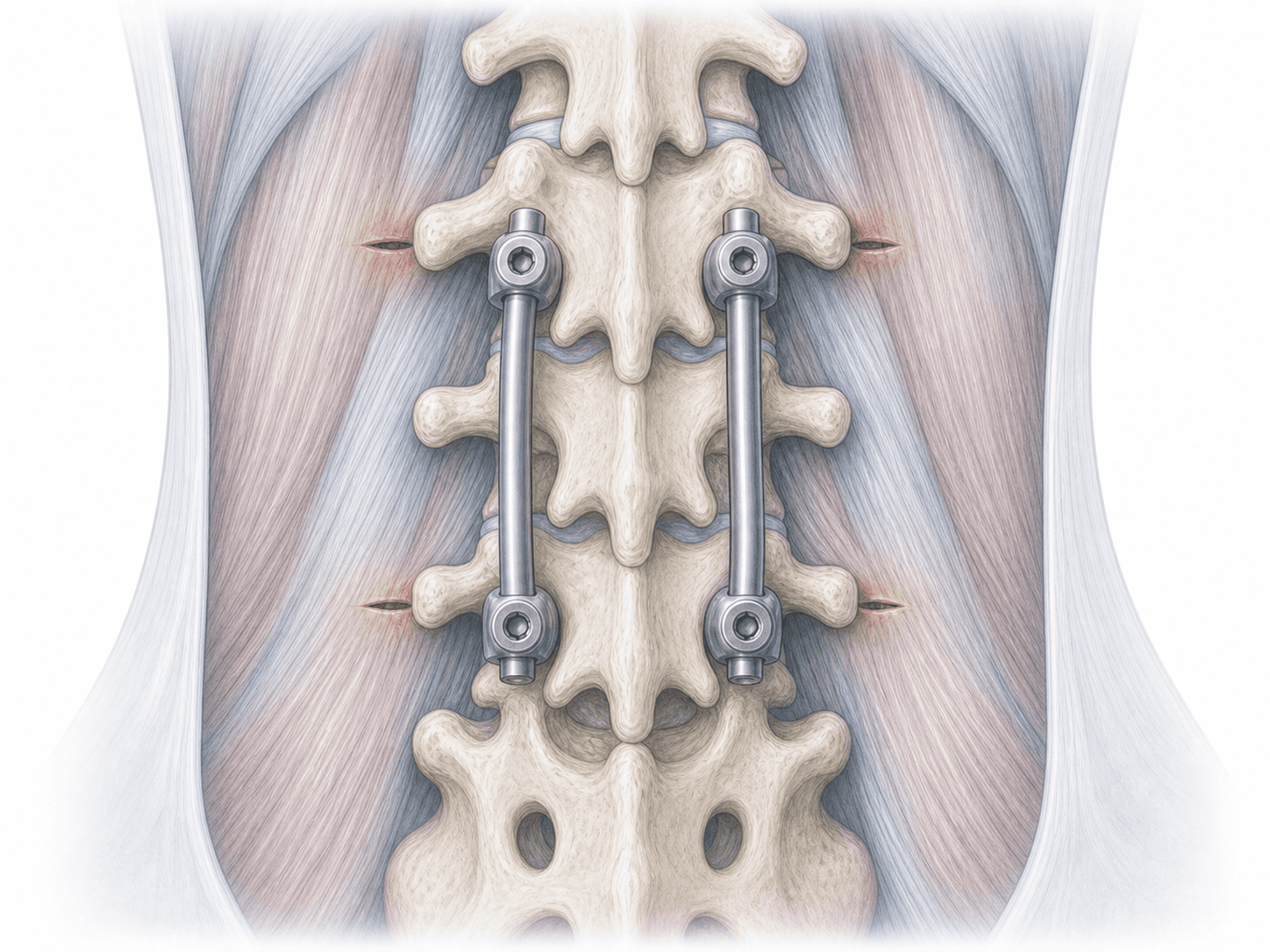
The procedure is performed under general anaesthesia. The vascular surgeon opens the abdominal wall and gently retracts the peritoneum, ureters and great vessels (aorta, vena cava, iliac vessels) to expose the anterior aspect of the disc. We remove the diseased disc, prepare the endplates and place an interbody cage, usually with bone graft, that restores disc height and lordosis. Depending on the case we add an anterior plate with screws or combine with posterior percutaneous fixation in a separate stage.
3.Immediate postoperative period
After surgery you spend time in the recovery unit and then return to your room. We monitor blood pressure, pain control, bowel function and leg pulses closely. Mobilisation begins within a few hours with the physiotherapist and, if progress is favourable, oral intake is resumed gradually. Hospital stay is usually 2–4 days.
Recovery after ALIF
Recovery is gradual. In the first weeks we focus on daily walking, pain control and protecting the abdominal wound. Return to sedentary work is usually considered between 4 and 8 weeks; physical or load-bearing jobs require longer.
Bony fusion consolidates over several months, so we recommend avoiding heavy lifting and impact early on and reintroducing activity under physiotherapy guidance. Fever, worsening abdominal or lumbar pain, leg swelling or any new neurological deficit warrant prompt medical review.
Risks and possible complications
Every surgery carries general risks such as infection, bleeding, thrombosis or anaesthesia-related complications.
ALIF has specific risks linked to the anterior approach: injury to the great vessels (aorta, vena cava, iliac vessels), transient paralytic ileus, peritoneal or ureteral injury and, in men, retrograde ejaculation due to involvement of the prevertebral sympathetic plexus. Non-union (pseudarthrosis), cage subsidence and accelerated degeneration of adjacent levels are also possible. These risks are assessed individually with the multidisciplinary team and minimised with careful vascular planning.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala