Tubular minimally invasive spine surgery
Tubular minimally invasive spine surgery is not a specific operation but a way of operating. We use sequential dilators that split the muscle fibres rather than cutting them, and we seat a working tubular retractor on top through which the procedure is performed under the microscope. This approach is used for lumbar microdiscectomy, stenosis decompression and even single-level fusion (MIS-TLIF). The goal is always the same: perform the same surgery we would do open, while sparing the tissues we pass through on the way to the spine. This guide explains when we use this technique, what its advantages are, where its limits lie and what recovery looks like.
What is tubular minimally invasive spine surgery?
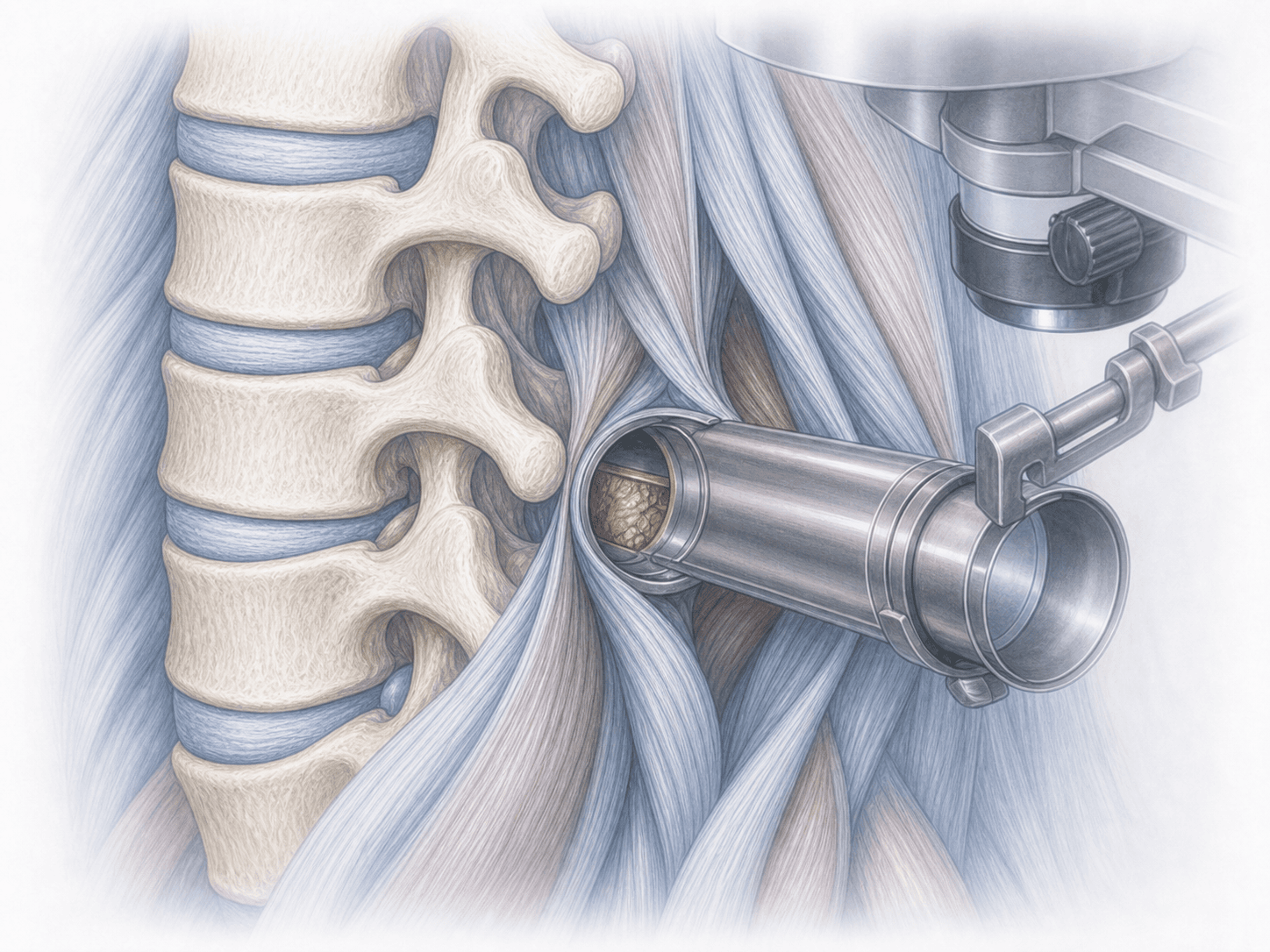
Tubular minimally invasive (MIS) spine surgery is a cross-cutting surgical technique. It is not a specific procedure but a way of reaching the spine that we apply to several different operations. Through a small skin incision, typically 18 to 26 mm, we introduce a thin dilator that gently spreads the paraspinal muscle fibres along the Wiltse plane. Over that first dilator we slide progressively wider ones and finally seat a working tube fixed to the operating table. Inside that tube, and always under the microscope, we perform the surgery.
The technique relies on tubular systems such as METRx, Quadrant or Spotlight, and we use it for lumbar microdiscectomy, over-the-top laminotomies for stenosis, foraminotomies or single-level fusions such as MIS-TLIF.
A key point: this is not about doing less surgery, but about doing the same surgery while sparing the muscle and soft tissues we pass through. If you want to know whether your case fits this approach, you can request an assessment with Dr. Ben Ghezala.
When we choose the tubular MIS technique
Because this technique does not treat a specific symptom but is a way of operating, what matters is knowing in which clinical scenarios we tend to choose it:
Surgical indications for tubular systems
How tubular MIS surgery is performed step by step
1.Preoperative preparation
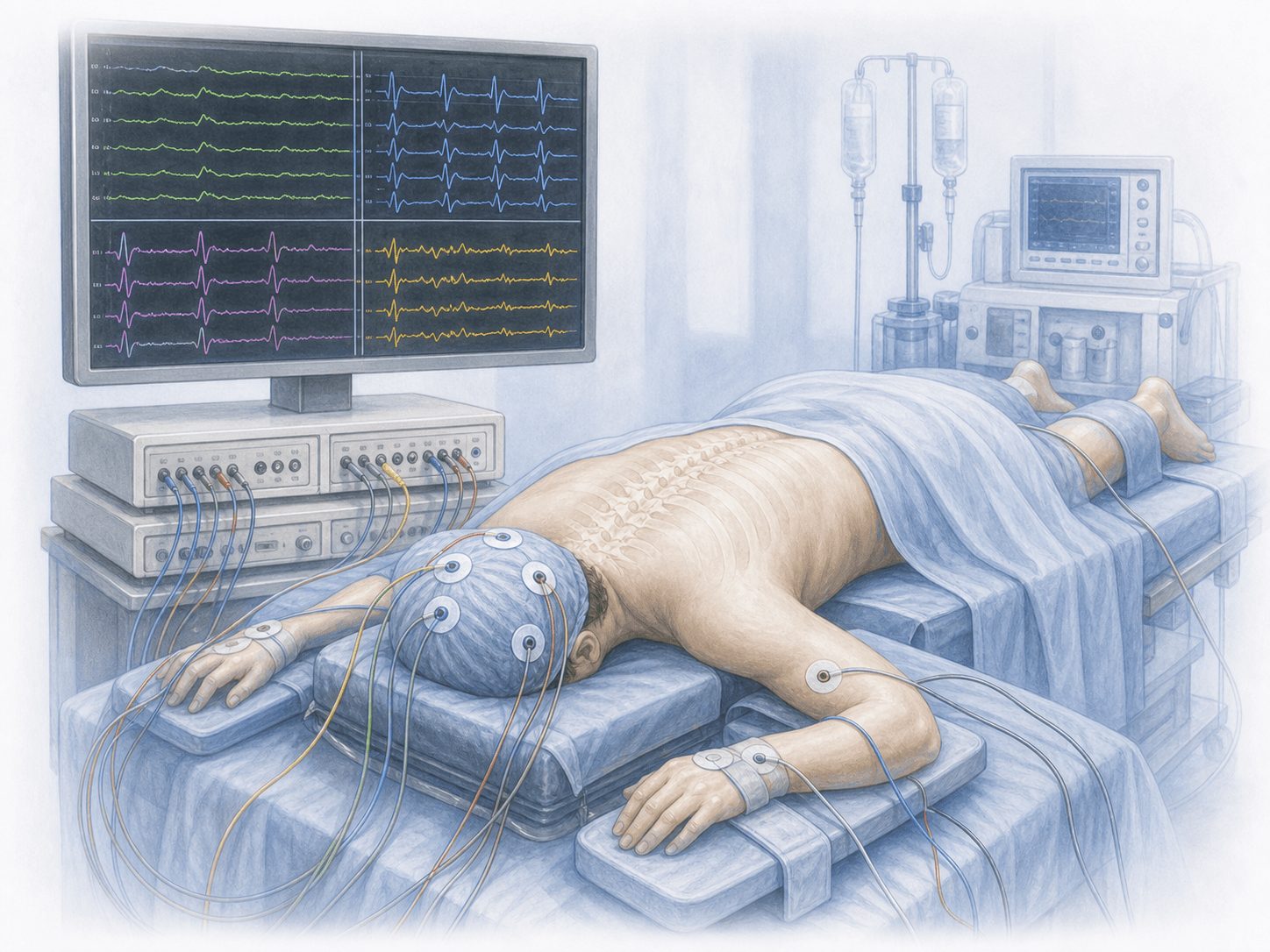
Before the procedure we review the MRI and, when needed, a dynamic X-ray to confirm the level and rule out instability. We explain why a tubular approach is the right fit in your case and which specific surgery we will perform through it. You will receive fasting instructions, medication adjustments (especially anticoagulants) and a preoperative blood test. Anaesthesia is general; the anaesthetist assesses you in advance.
2.During the surgery
With the patient prone on the operating table, we localise the level with fluoroscopy and make a small incision lateral to the midline. We introduce a first thin dilator that splits the paraspinal muscle without cutting it and slide progressively wider dilators over it. A working tube is then seated and fixed to an articulated arm anchored to the table.
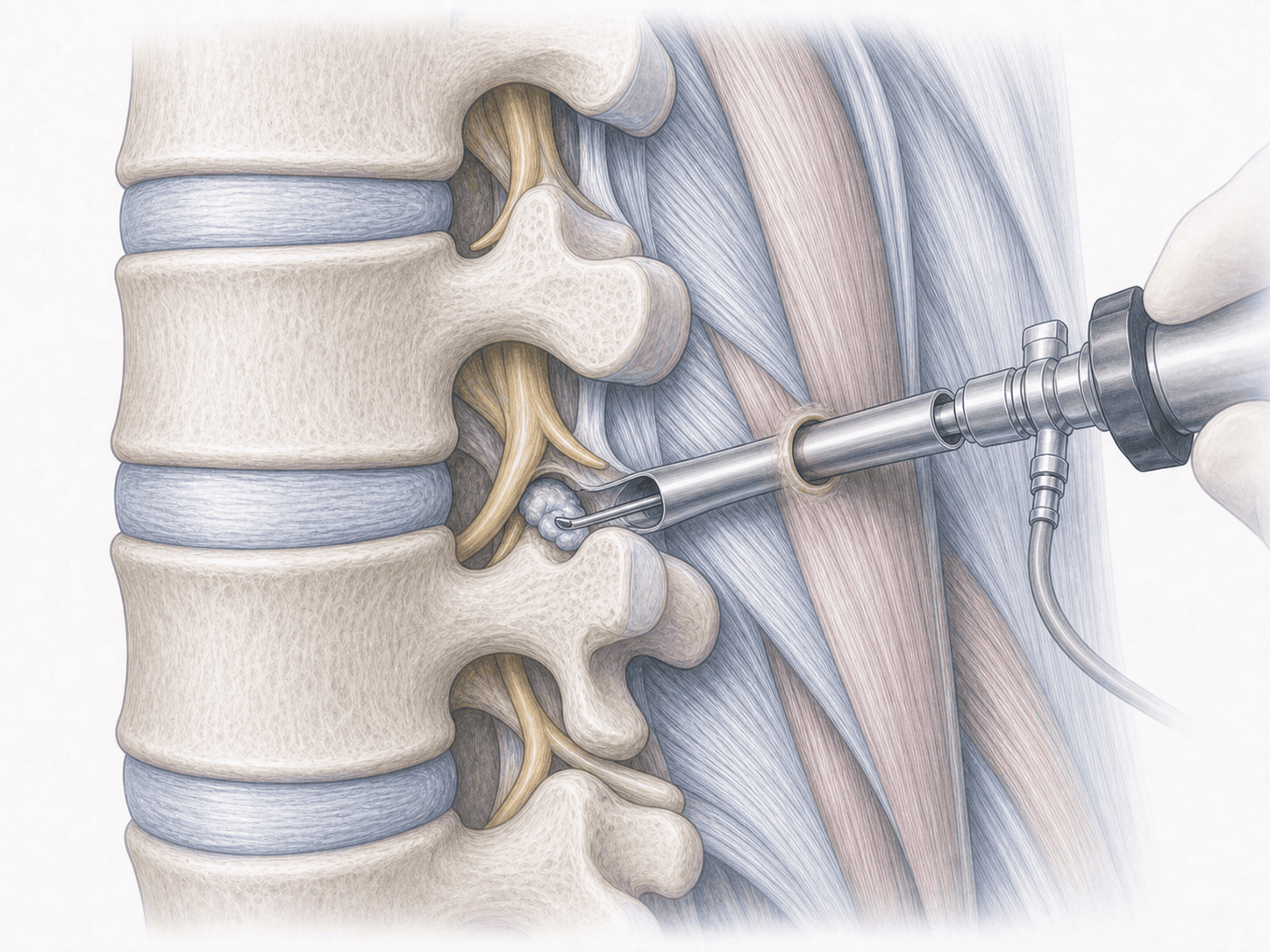
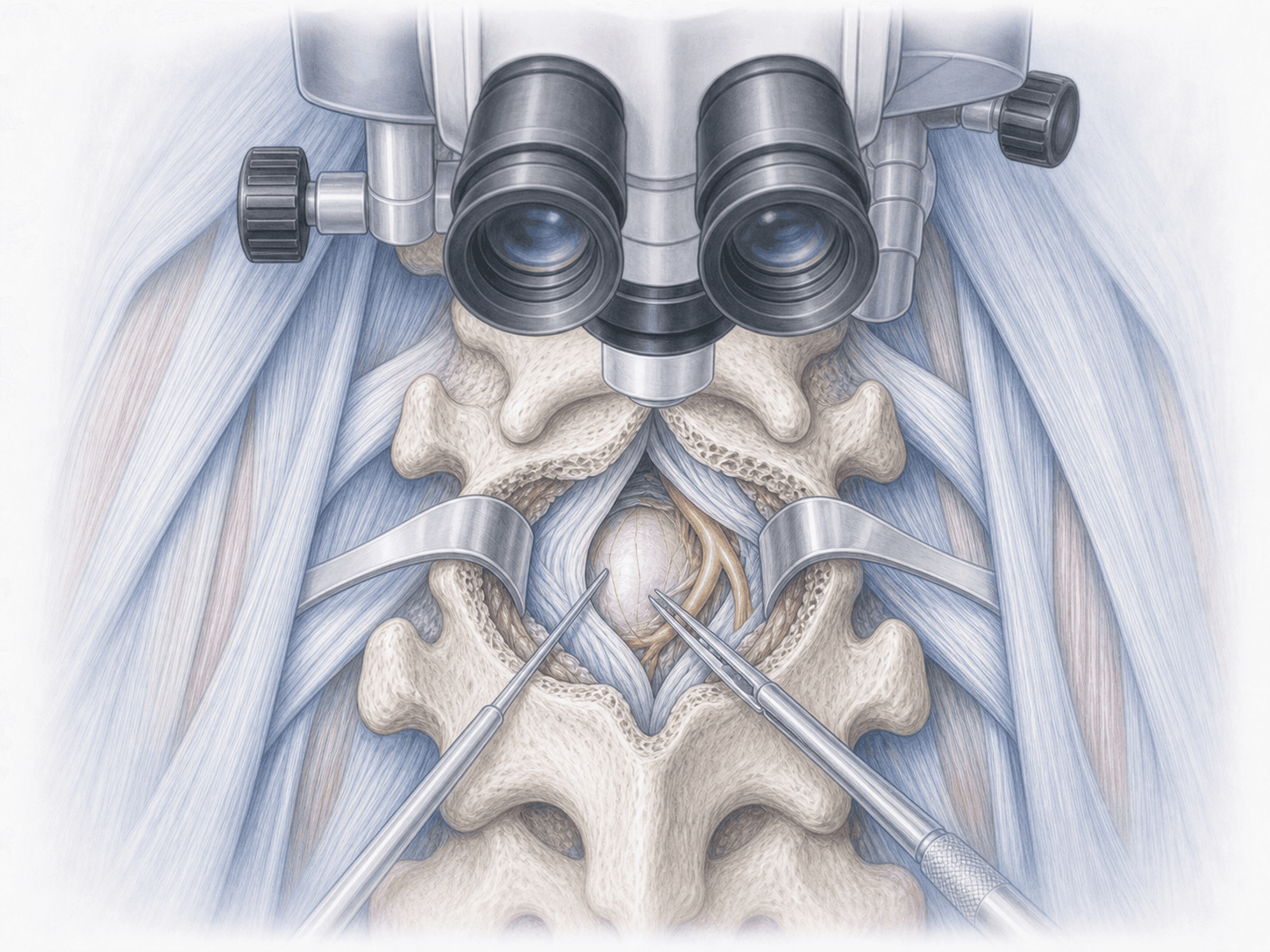
The surgical microscope is mounted over the tube. Through it we perform the planned surgery: removing the herniated fragment, opening the ligamentum flavum and decompressing the canal, widening the foramen or, in a MIS-TLIF, preparing the disc space, inserting an interbody cage and completing the construct with percutaneous pedicle screws. At the end we remove the tube: the muscle returns to its position and the skin incision is closed with only a few stitches.
3.Immediate postoperative period
On waking, back pain is usually much milder than after open surgery on the same segment, because the muscle has not been cut. After microdiscectomy or simple decompression many patients walk the same afternoon or the next morning. Hospital stay is typically 24 hours for decompressive procedures and 24 to 48 hours for MIS-TLIF, always adjusted to clinical progress.
Recovery after tubular MIS surgery
Recovery is one of the strongest arguments for this technique. Because the paraspinal muscle is not detached, postoperative back pain is lower and independent walking resumes very early. Daily activities are typically resumed within a few days and office work within 2 to 3 weeks after simple decompression; MIS-TLIF takes somewhat longer.
In the first weeks we ask patients to avoid heavy lifting, sustained flexed postures and impact sports. Physiotherapy starts gradually, usually between the second and fourth week. Bony fusion, when performed, still needs several months to consolidate even though the immediate postoperative course is gentler.
Fever, worsening pain, new weakness or wound drainage warrant prompt medical review.
Risks and possible complications
The tubular technique reduces muscle damage and blood loss, but it does not eliminate the risks of operating on the spine.
General risks include infection, bleeding, anaesthesia-related issues or thrombosis. Risks specific to working through a narrow corridor include cerebrospinal fluid leak from a dural tear, nerve root injury, incomplete decompression if the field does not reach the whole pathology, and a small risk of conversion to open surgery. In MIS-TLIF we add the risks tied to instrumentation: screw malposition, non-union (pseudarthrosis) or adjacent segment degeneration. The technique also carries a real learning curve; we use it routinely.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala