Endoscopic spine surgery
Full-endoscopic spine surgery (FESS) is a minimally invasive technique we use to treat disc herniations and nerve root compressions in the cervical, thoracic or lumbar spine through an incision of around 7-8 millimetres. We work with a spinal endoscope and a dedicated working channel under continuous irrigation, providing a direct, magnified view of the disc and nerve root without retracting muscle or removing significant amounts of bone. It is one of the most tissue-sparing techniques available: most patients are discharged the same day and walk within a few hours of surgery.
What is endoscopic spine surgery?
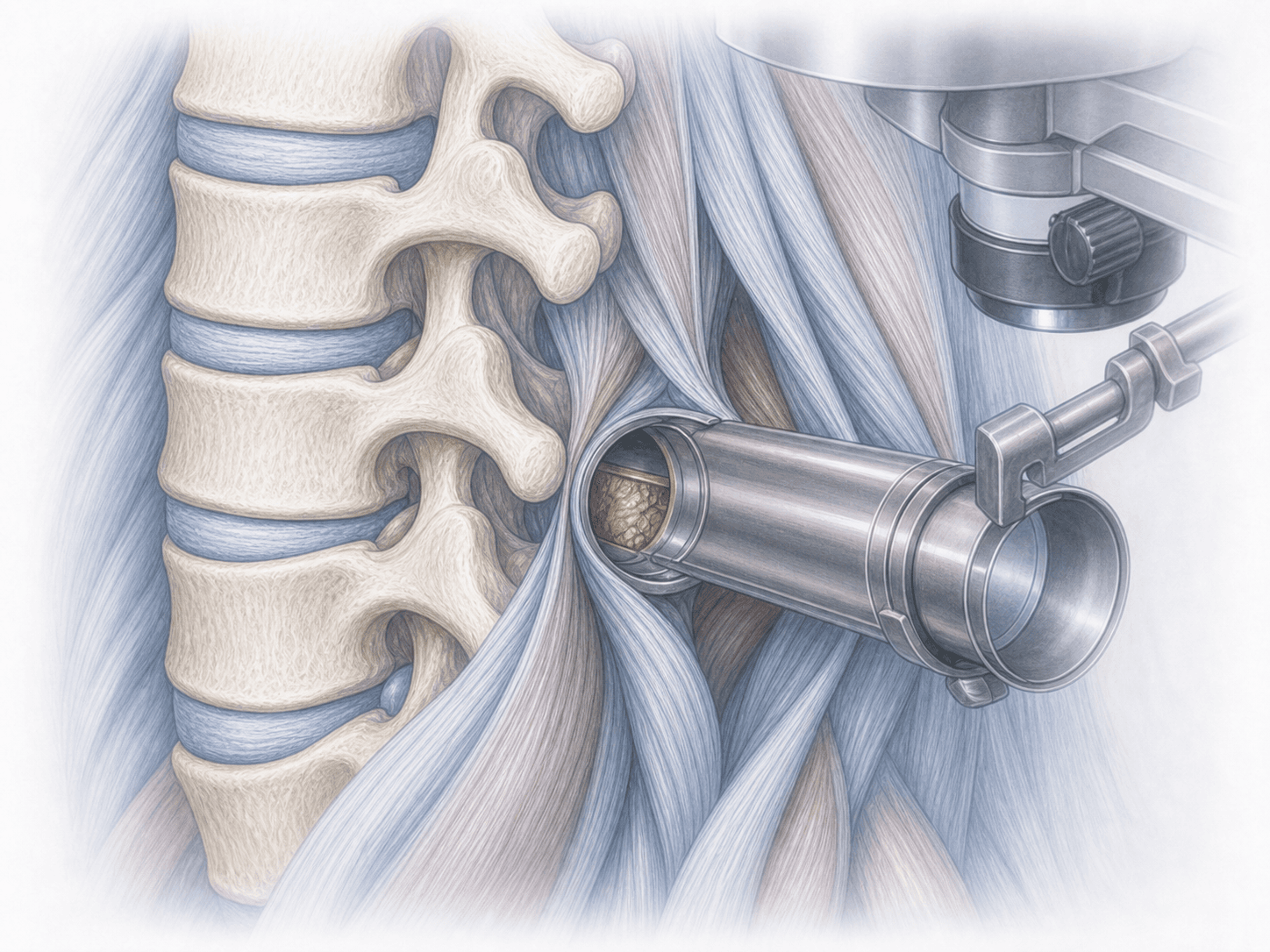
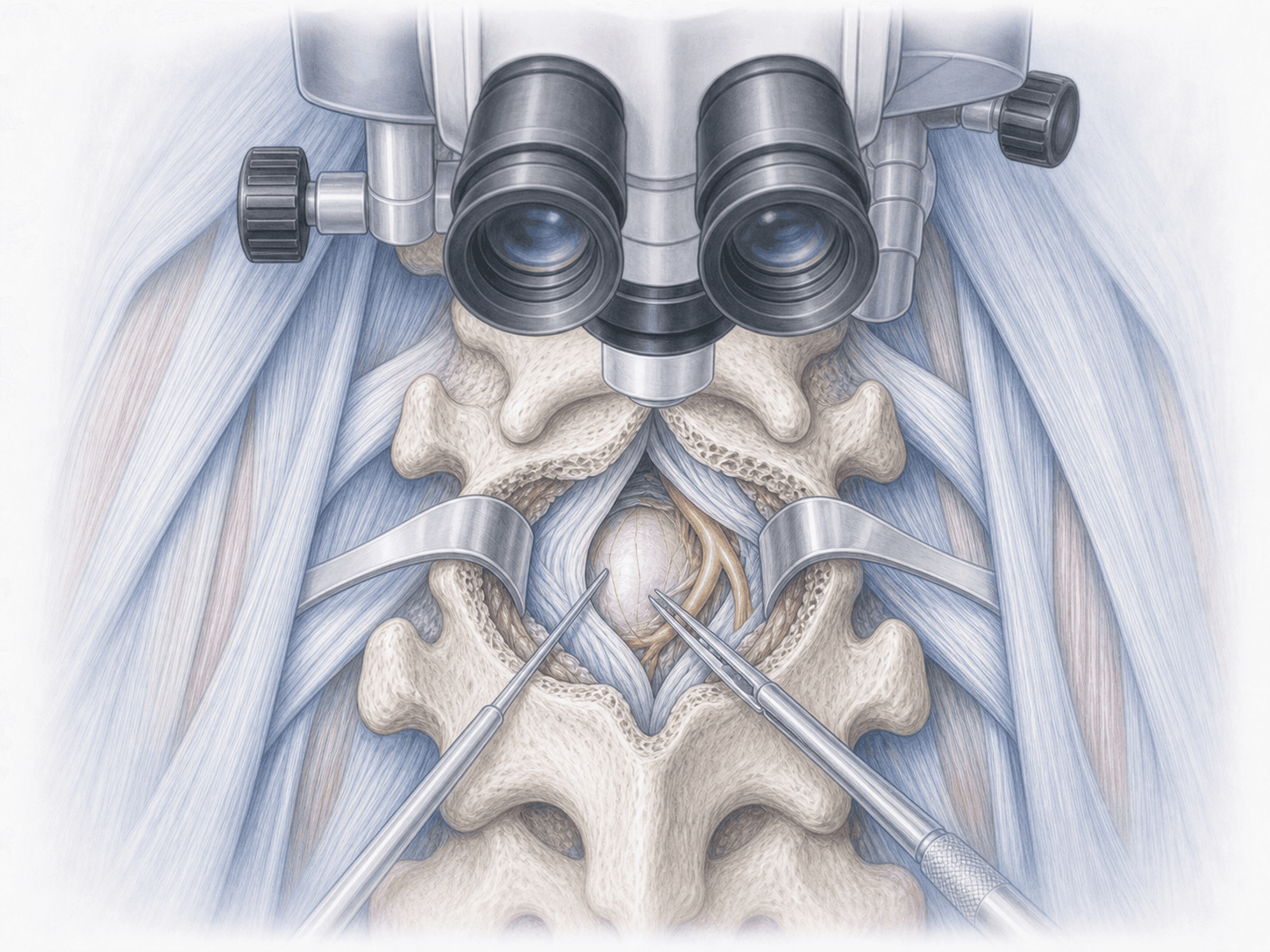
Endoscopic spine surgery is a minimally invasive procedure that uses a working-channel spinal endoscope to treat disc herniations and nerve compressions in the cervical, thoracic or lumbar spine. Through an incision of around 7-8 millimetres we introduce the endoscope under continuous saline irrigation, which keeps the surgical field clean and provides a direct, high-definition view of the disc, the nerve root and the ligamentum flavum.
Unlike open surgery or tubular minimally invasive surgery, the paraspinal muscles are not split with wide retractors and bone removal is kept to a minimum. Depending on the pathology we choose a transforaminal, interlaminar or posterolateral approach, and in many cases the procedure can be performed under local anaesthesia with sedation, with the patient awake and cooperating. To discuss whether your case is suitable for this approach, you can request an assessment with Dr. Ben Ghezala. For isolated lumbar disc herniations the endoscopic lumbar discectomy is usually our reference technique.
When it applies: typical clinical scenarios
Endoscopic spine surgery is offered to patients with clear signs of nerve compression that have not improved with conservative treatment. The most frequent clinical scenarios are:
When is this technique indicated?
How is the procedure performed?
1.Preoperative preparation
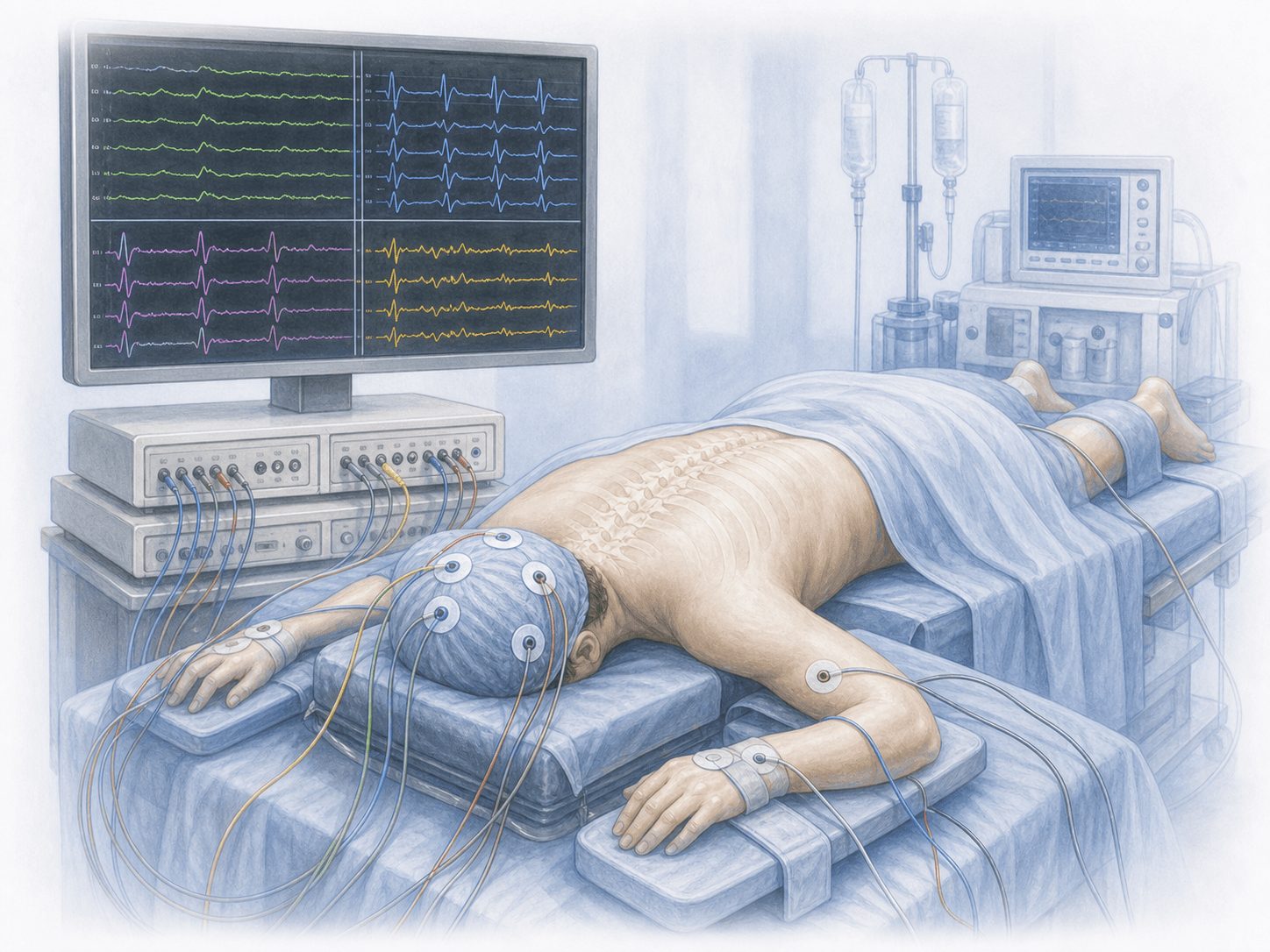
We review your MRI together and, when needed, dynamic X-rays to rule out instability. We confirm the level to be treated, plan the approach (transforaminal, interlaminar or posterolateral) and choose the anaesthetic: local with sedation for most lumbar cases and general anaesthesia for posterior cervical approaches. You receive clear fasting instructions, adjustments to any anticoagulant or antiplatelet medication and the opportunity to clarify any concerns before the day of surgery.
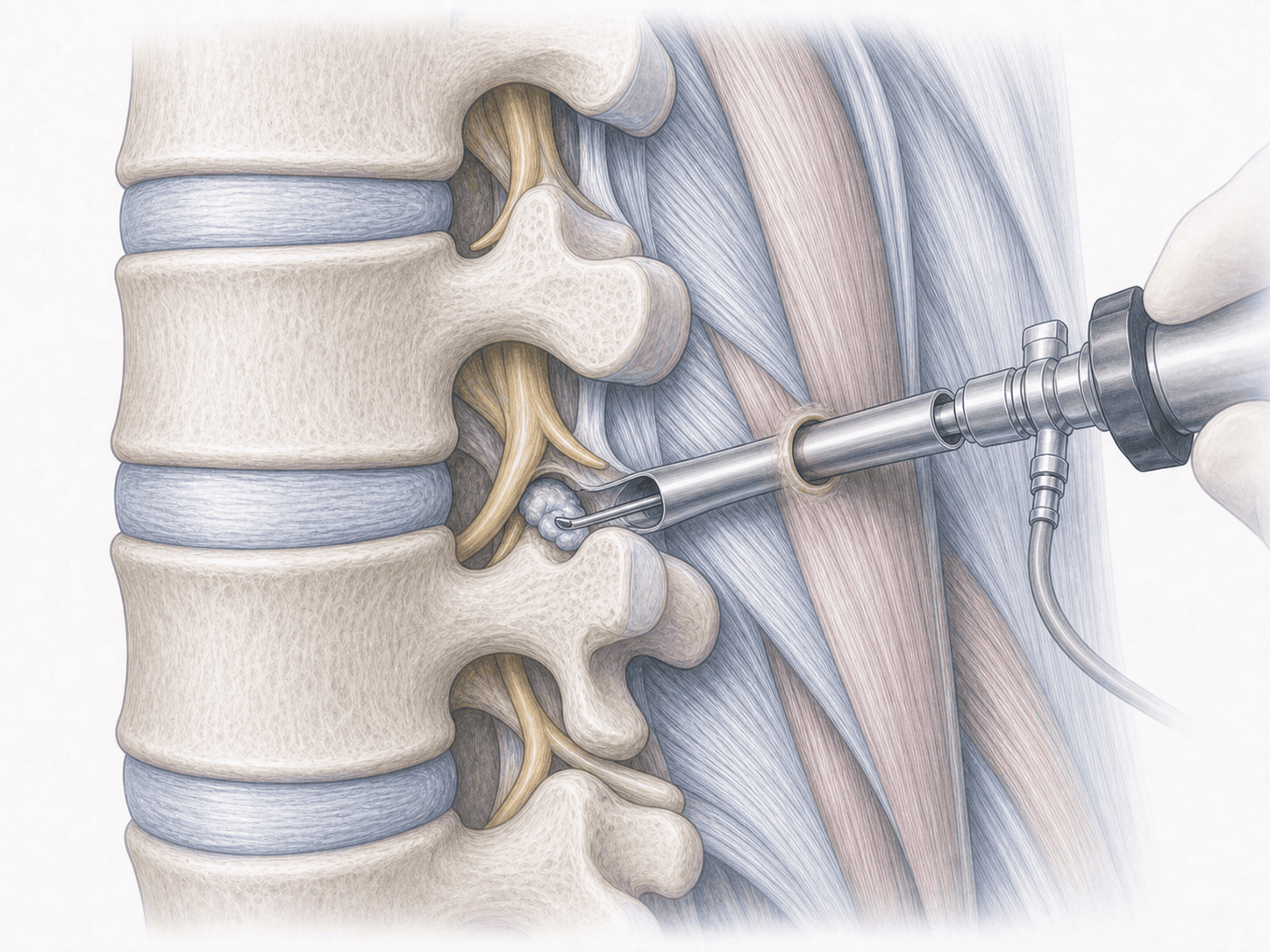
2.During the procedure
With the patient in prone or lateral position, we mark the entry point under fluoroscopic guidance and perform a 7-8 millimetre incision. We gradually dilate the soft tissues until we reach the epidural or foraminal space and advance the endoscope with its working channel. From there, under continuous saline irrigation, we remove the herniated fragment, enlarge the foramen if foraminal stenosis is present and confirm complete decompression of the nerve root before removing the endoscope. The wound is closed with one or two sutures.
3.Immediate postoperative period
After surgery you spend a few hours in recovery or observation. Walking and oral intake usually start within hours. In most lumbar herniations we discharge patients the same day; in selected cases with general anaesthesia or comorbidities a single overnight stay is enough. You leave with a clear pain-control plan, wound-care instructions and a phased return-to-activity programme.
Recovery after endoscopic spine surgery
Recovery is usually fast compared with open surgery. During the first days we encourage frequent short walks, no heavy lifting and careful wound protection. Most patients with office-based jobs return between 1 and 3 weeks; physically demanding jobs need a longer, individualised window.
Physiotherapy is introduced gradually once the wound has closed. Postural ergonomics and structured core strengthening are key to maintaining the long-term result. Fever, persistent pain, new weakness or any bowel or bladder changes require immediate medical review.
Risks and possible complications
Every surgery carries general risks such as infection, bleeding, thrombosis or anaesthesia-related complications, although these are less frequent in endoscopic surgery thanks to the small incision.
Specific risks include transient nerve root irritation with paraesthesia or dysaesthesia, cerebrospinal fluid leak from dural tear, recurrent herniation at the same level and incomplete decompression that may require conversion to an open technique. Careful patient selection, approach planning and the surgeon's experience are the main factors that reduce these complications.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala