Cervical kyphosis correction
Cervical kyphosis correction is a surgery designed to restore neck balance when the spine loses its natural curve and tilts forward. Many patients reach our clinic with a neck that cannot hold itself up, persistent pain, difficulty looking ahead or neurological symptoms from spinal cord compression after previous surgery, ankylosing spondylitis or advanced degeneration. At our practice in Alicante and Benidorm we assess every case with dynamic imaging, 3D planning and an individualised surgical plan to realign the neck as safely as possible.
What is cervical kyphosis correction?
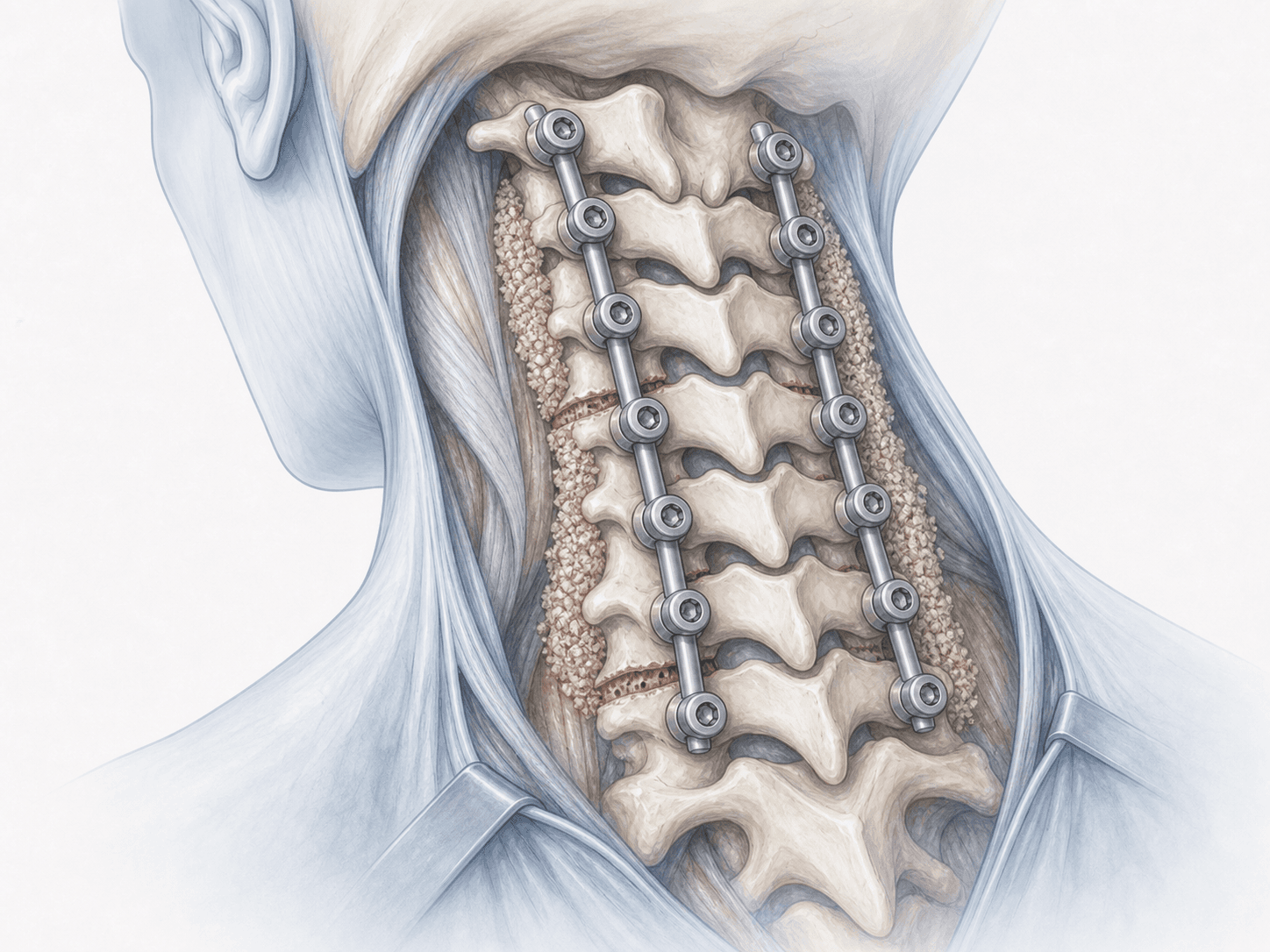
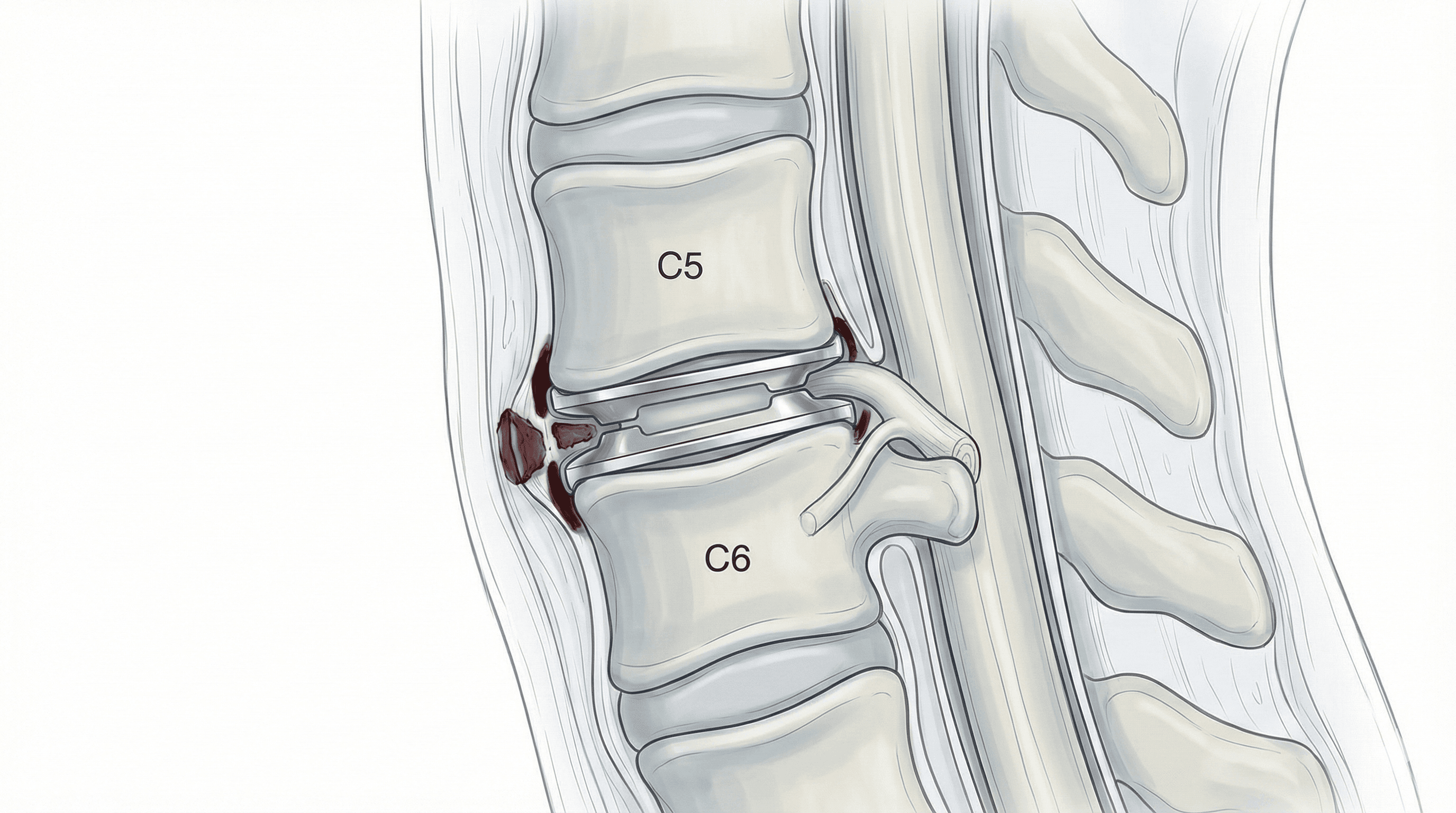
Cervical kyphosis correction is a surgery aimed at restoring the natural curve of the neck when it has been lost and the spine tilts forward. Depending on the stiffness and the size of the deformity, we combine decompression, osteotomies and instrumentation with screws and rods to restore sagittal balance across the C2-C7 segment.
Flexible kyphosis can sometimes be addressed with posterior cervical fusion or a multilevel ACDF. Fixed kyphosis, usually linked to ankylosing spondylitis or extensive previous laminectomies, often requires a combined anterior-posterior approach with Smith-Petersen or pedicle subtraction osteotomies. To discuss your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients with symptomatic cervical kyphosis usually describe:
When is this surgery indicated?
How is the procedure performed?
1.Preoperative preparation
Before surgery we complete a full work-up: MRI, CT with 3D reconstruction, dynamic flexion-extension X-rays and a full-spine standing radiograph to measure sagittal balance. We assess how rigid the deformity is, plan the levels to instrument and review your medication, fasting and preoperative tests.
2.During the procedure
Surgery is performed under general anaesthesia with continuous neurophysiological monitoring (motor and sensory evoked potentials). For flexible kyphosis we typically use an anterior approach with multilevel discectomies, interbody cages and a plate. For rigid kyphosis we combine an anterior release with a posterior stage involving osteotomies (Smith-Petersen or pedicle subtraction) and instrumentation with lateral mass and pedicle screws. Realignment is done in a controlled fashion to protect the spinal cord and nerve roots.
3.Immediate postoperative period
After surgery you will spend a few hours in recovery with close neurological monitoring. Once stable you return to the ward. Gentle mobilisation with a collar starts on day one and pain is managed with a multimodal protocol. Hospital stay is usually 3 to 7 days depending on the complexity of the correction.
Recovery after cervical kyphosis correction
Recovery after a cervical correction is longer than after a simple cervical surgery because osteotomies and multilevel instrumentation are involved. The first 2-3 weeks focus on wound care, walking and postural hygiene, with a collar when indicated.
At 4-6 weeks most patients resume daily activities and driving when we authorise it. Office work usually restarts between 6 and 12 weeks, whereas physical jobs need 3 to 6 months. Fusion consolidates over several months, so we avoid heavy strain early on and plan rehabilitation for the neck and posterior muscles.
Fever, wound discharge, new severe pain or any neurological change should be reviewed immediately.
Risks and possible complications
Every surgery carries general risks such as infection, bleeding, thrombosis or anaesthetic complications. Cervical kyphosis correction is major surgery and the specific risks deserve an honest explanation.
The most relevant ones are injury to the spinal cord or nerve roots during realignment, hardware loosening or failure, pseudarthrosis (non-union), transient or prolonged dysphagia, vascular injury, proximal or distal junctional kyphosis and the need for revision surgery. This is why we use continuous neurophysiological monitoring and 3D planning, and why we reserve this surgery for carefully selected cases.
Frequently asked questions
Other related treatments



Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala