Failed spinal instrumentation revision
Revision of a failed spinal instrumentation is considered when hardware placed in a previous surgery (pedicle screws, rods, plates or interbody cages) has broken by fatigue, loosened due to non-fusion or ended up malpositioned, causing mechanical pain, neurological symptoms or a risk of structural damage. We understand how distressing it is to learn that the hardware meant to stabilise your spine is now part of the problem. We offer a careful second-opinion assessment, reviewing the previous operative report, your current imaging and your clinical course to understand what has failed and what can be done. This guide summarises the most frequent causes, how hardware failure is diagnosed and which options exist: from partial or complete removal of the implants to re-instrumentation with larger-diameter screws, cement-augmented screws or a longer construct.
What is failed spinal instrumentation revision?
Revision of a failed spinal instrumentation is a salvage operation aimed at correcting problems with hardware placed in a previous spine surgery: pedicle screws broken by fatigue, fractured rods, loosening of the bone anchor, subsided interbody cages or malpositioned screws that invade the spinal canal, foramen or vertebral wall.
Unlike a straightforward hardware removal, this surgery first analyses why the instrumentation failed (pseudarthrosis, mechanical overload, stress fracture, low-grade chronic infection) and then decides between removing the hardware, replacing it or extending the construct. To review your specific case you can request a second opinion with Dr. Ben Ghezala, a German-trained spine neurosurgeon.
Symptoms and signs of hardware failure
Patients with failing instrumentation typically report:
When is instrumentation revision indicated?
How is the procedure performed?
1.Preoperative preparation
Before planning the revision we request a thin-slice CT to identify breakage, loosening and screw trajectories, an MRI to assess the soft tissues and rule out infection, and dynamic X-rays to confirm instability. The previous operative report and the exact implant brand are reviewed so the proper removal instruments can be prepared. If infection is suspected, laboratory tests (CRP, ESR, blood cultures) are completed and intraoperative sampling is planned.
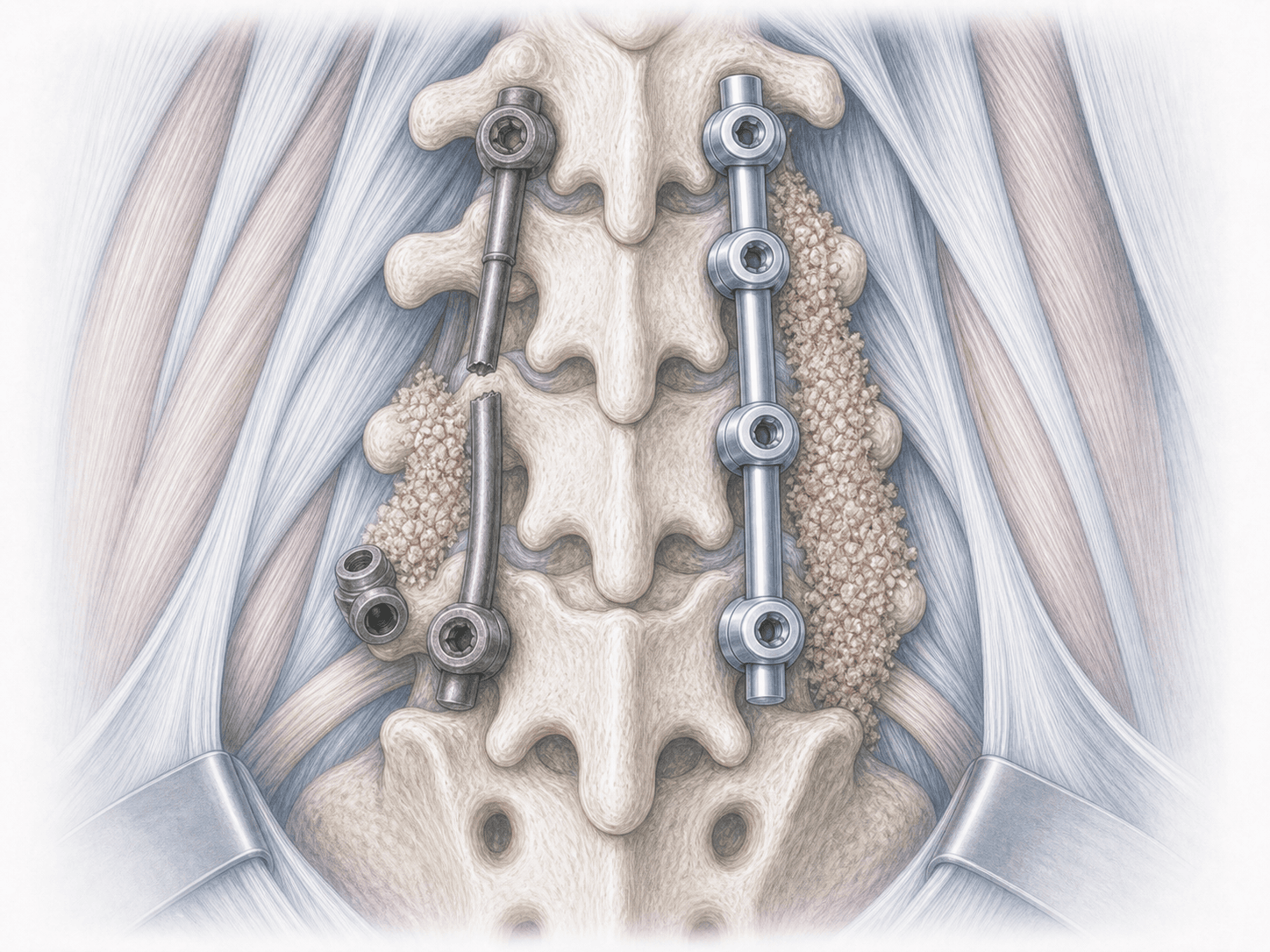
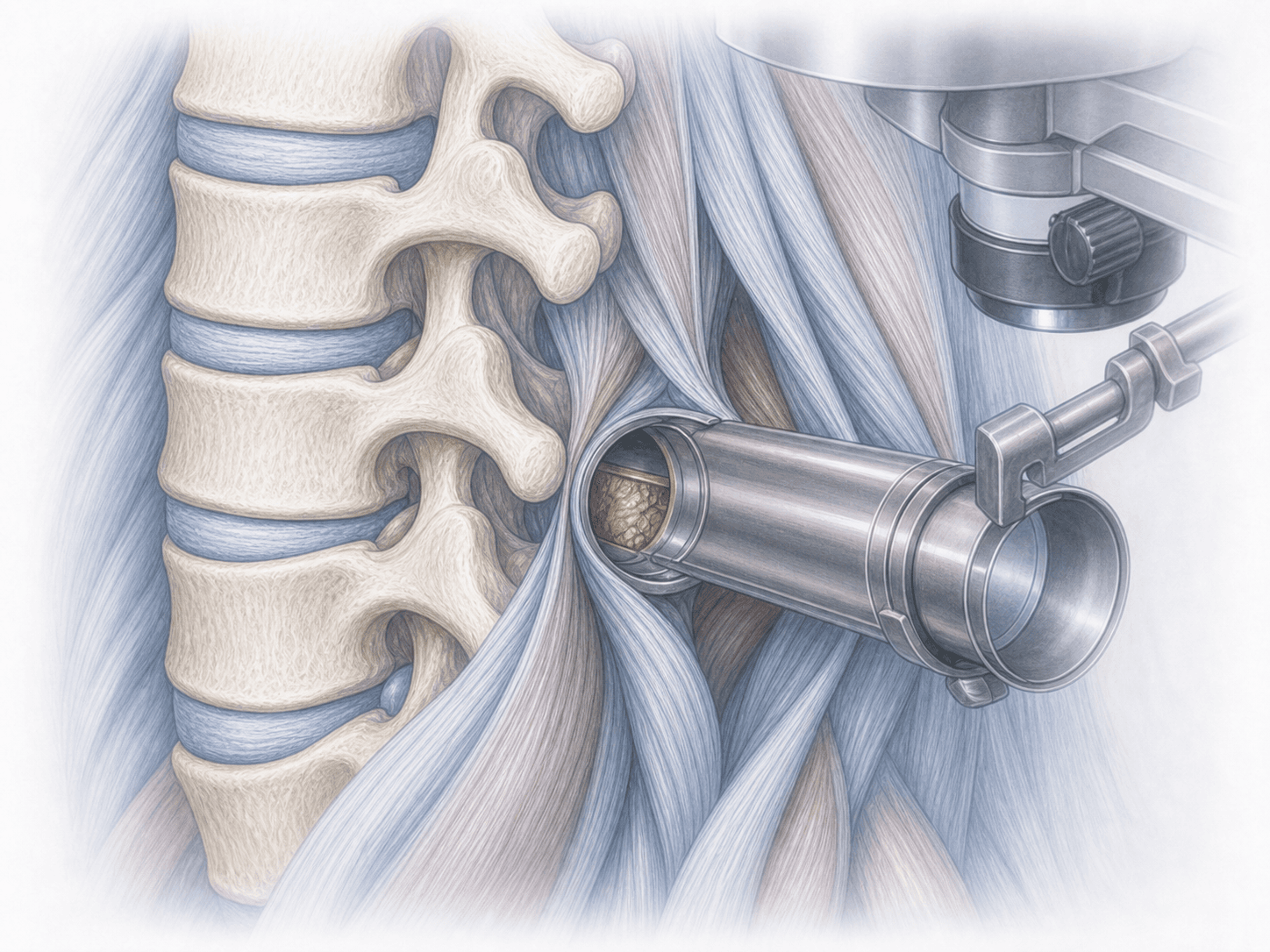
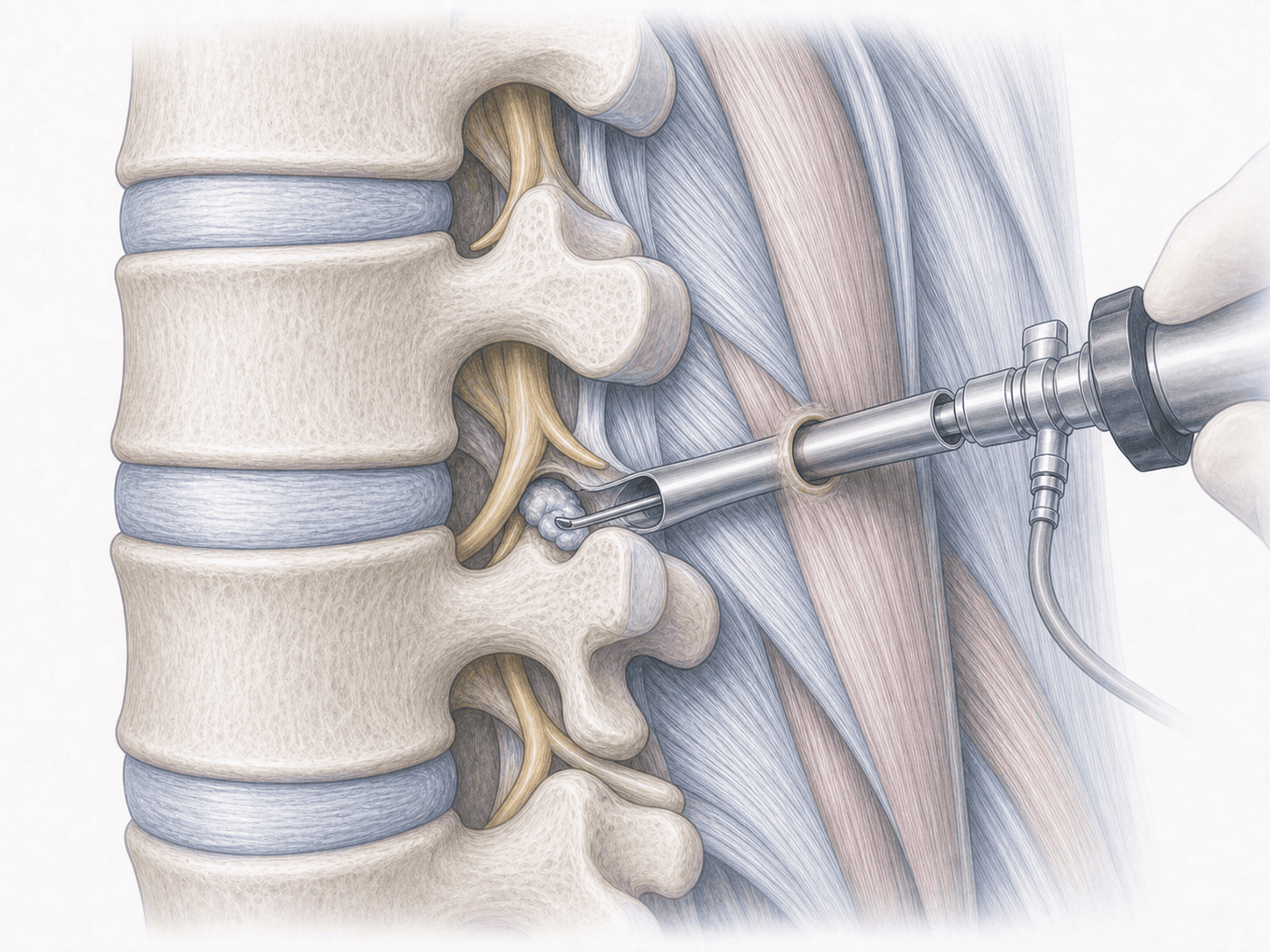
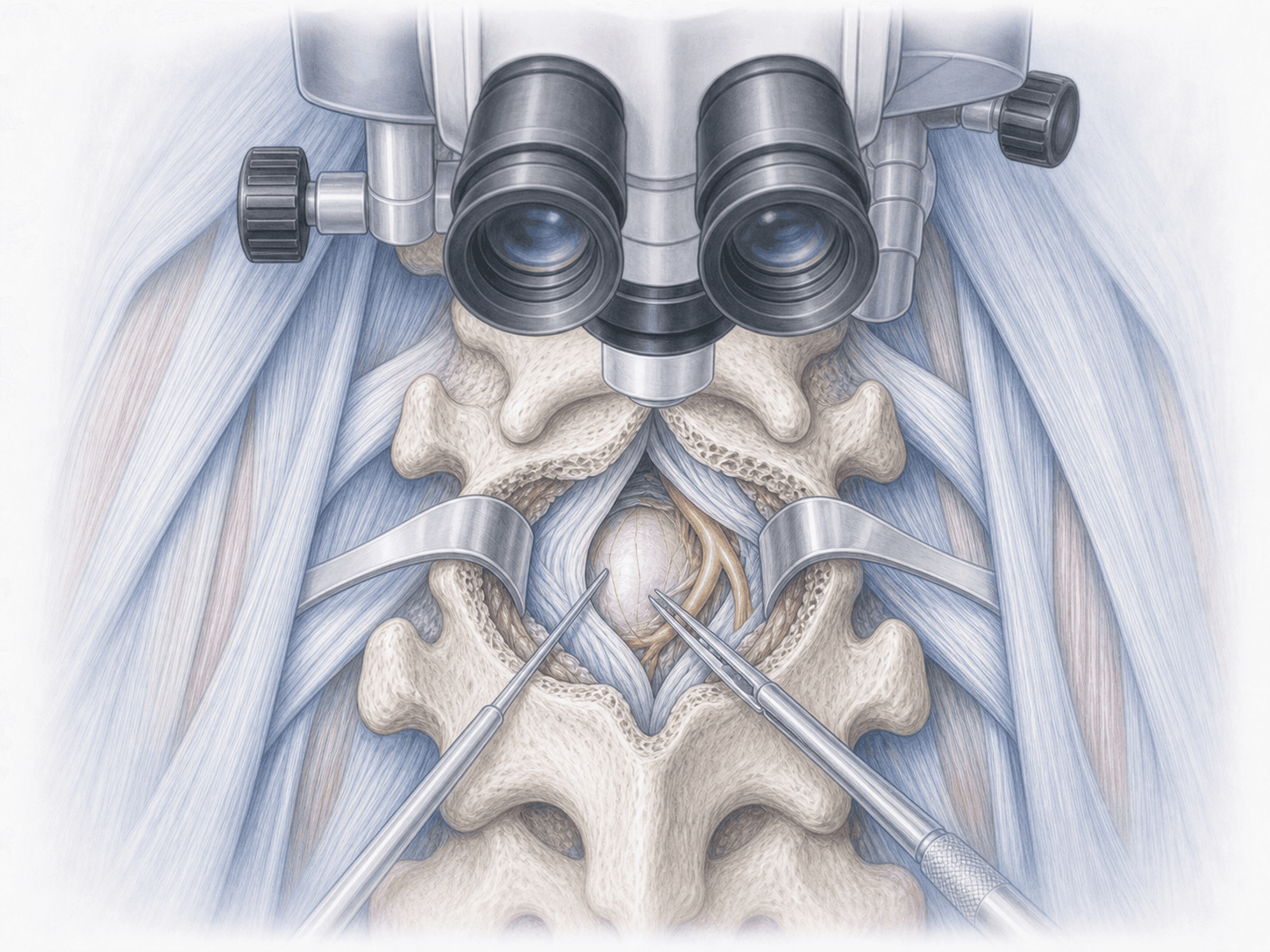
2.During the procedure
The approach is usually performed through the previous scar, with careful dissection to avoid injuring the dura and the scarred nerve roots. The broken or loose hardware is identified and removed, cultures are taken if appropriate and the bony bed is assessed. If fusion has consolidated and the hardware is no longer needed, it is simply removed. If pseudarthrosis or instability persists, the segment is re-instrumented with larger-diameter screws, cement-augmented screws in osteoporotic bone, or the construct is extended to an adjacent level. When required, bone graft is added and the subsided cage is replaced.
3.Immediate postoperative period
Patients spend a few hours in recovery before returning to their room. Pain is controlled with multimodal analgesia and gradual mobilisation starts, usually on the first postoperative day. If infection was suspected, antibiotics are adjusted according to intraoperative culture results. Hospital stay is generally 3 to 6 days depending on the complexity of the revision and clinical response.
Recovery after instrumentation revision
Recovery is slower than after a first surgery because scar tissue is stiffer and the bone is often weakened. Light daily activities resume in 2–3 weeks. Return to office work usually takes 6 to 12 weeks, and physical jobs may require longer.
Bony consolidation after re-instrumentation takes several months, so heavy strain, sudden rotations and high axial load are avoided during the first three months. Rehabilitation is introduced gradually and always supervised. Fever, wound discharge, unexpectedly worsening pain or new neurological symptoms warrant prompt medical review.
Risks and possible complications
Any revision surgery carries more risks than a first operation. General risks include infection, bleeding, thrombosis and anaesthesia-related complications.
Specific risks include dural tears when releasing adhesions, injury to scarred nerve roots, pedicle fracture when extracting a tightly seated screw, failure of the new anchor in osteoporotic bone, persistence of pseudarthrosis and, if low-grade chronic infection is present, the need for a staged second procedure. These risks are reviewed individually and explained in detail before any decision is made.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala