Spondylodiscitis surgery
Spondylodiscitis is an infection of the intervertebral disc and the adjacent vertebral bodies that can destroy bone, create an epidural abscess and threaten spinal stability. Most cases are caused by Staphylococcus aureus, although tuberculosis (Pott disease) and brucellosis are also possible. Many patients arrive after weeks of severe back pain, fever or loss of strength, sometimes already on antibiotics without a clear response. The decision to operate is not automatic: it depends on neurological status, spinal stability, the causative organism and how the patient evolves on conservative treatment. This guide explains when surgery is needed, how it is performed and what to expect afterwards, with the calm and clinical urgency the condition demands.
What is spondylodiscitis surgery?
Spondylodiscitis is an infection of the intervertebral disc and the adjacent vertebral bodies. The most common organism is Staphylococcus aureus, although tuberculous (Pott disease) and brucellar forms are also seen, particularly in patients with relevant epidemiological background. Diagnosis combines contrast-enhanced MRI, blood cultures, CRP/ESR and, when needed, CT-guided biopsy to identify the pathogen.
Most cases are controlled with prolonged intravenous antibiotics (6–12 weeks) and relative rest. Surgery is considered when neurological deficit appears, when there is a significant epidural abscess, when instability or progressive deformity develops or when medical treatment fails. The surgical goal is to debride the infected focus, decompress neural structures and, if the spine has become unstable, fix the segment with an interbody cage and titanium screws.
In milder, well-selected cases a lumbar microdiscectomy may be considered first when the disease is focal, but advanced spondylodiscitis usually requires a wider approach. To review your case in detail, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Spondylodiscitis often presents in a slow, non-specific way and is therefore diagnosed late. The following signs should raise suspicion:
When is surgery indicated?
How is the surgery performed?
1.Preoperative preparation
Imaging studies (contrast-enhanced MRI, CT), blood cultures, CRP, ESR and, when available, biopsy results are reviewed. Targeted antibiotic therapy is adjusted whenever possible. Anaesthesia assesses general status and comorbidities (diabetes, immunosuppression) and prophylaxis, fasting and medication management are planned.
2.During the procedure
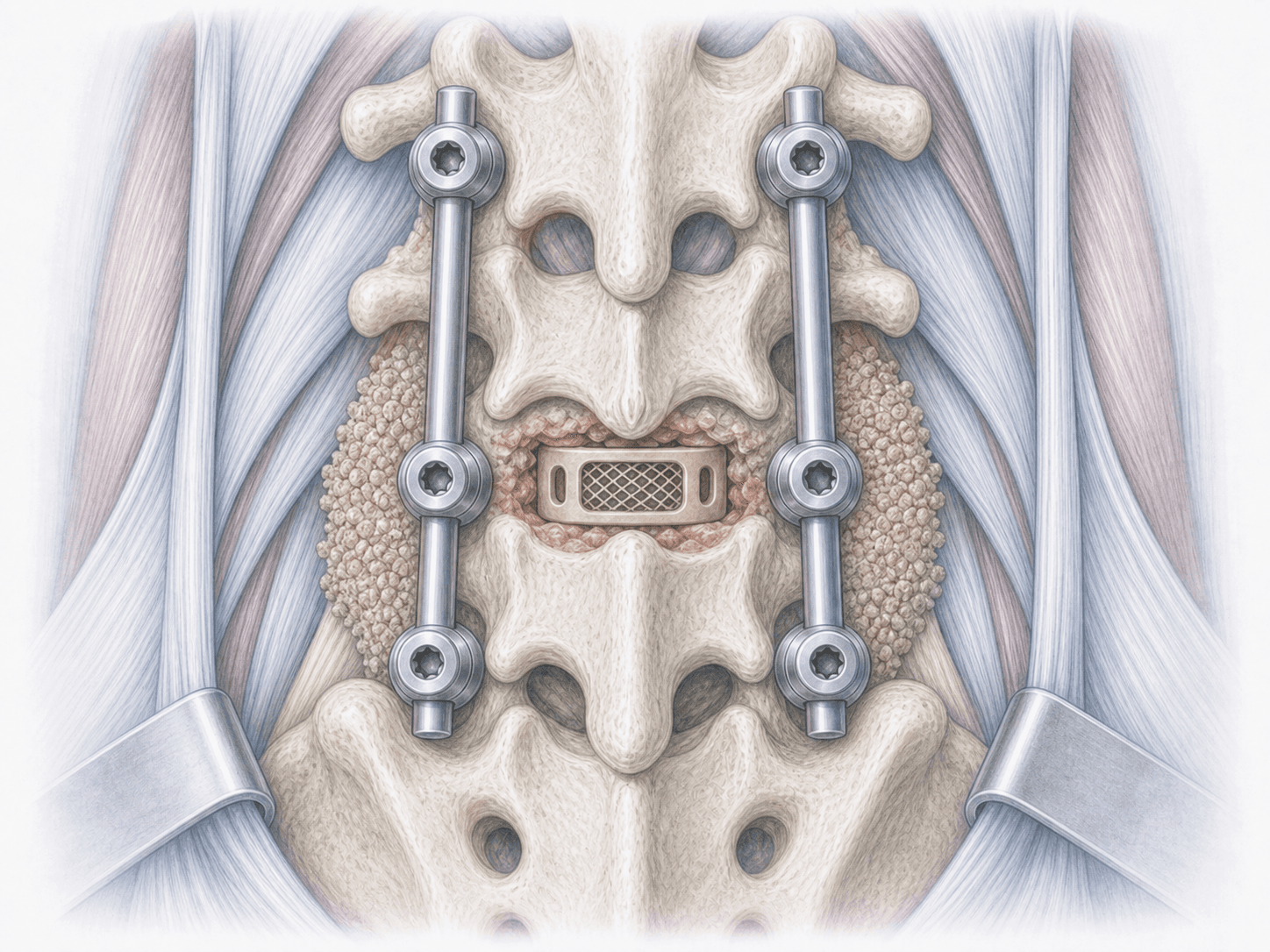
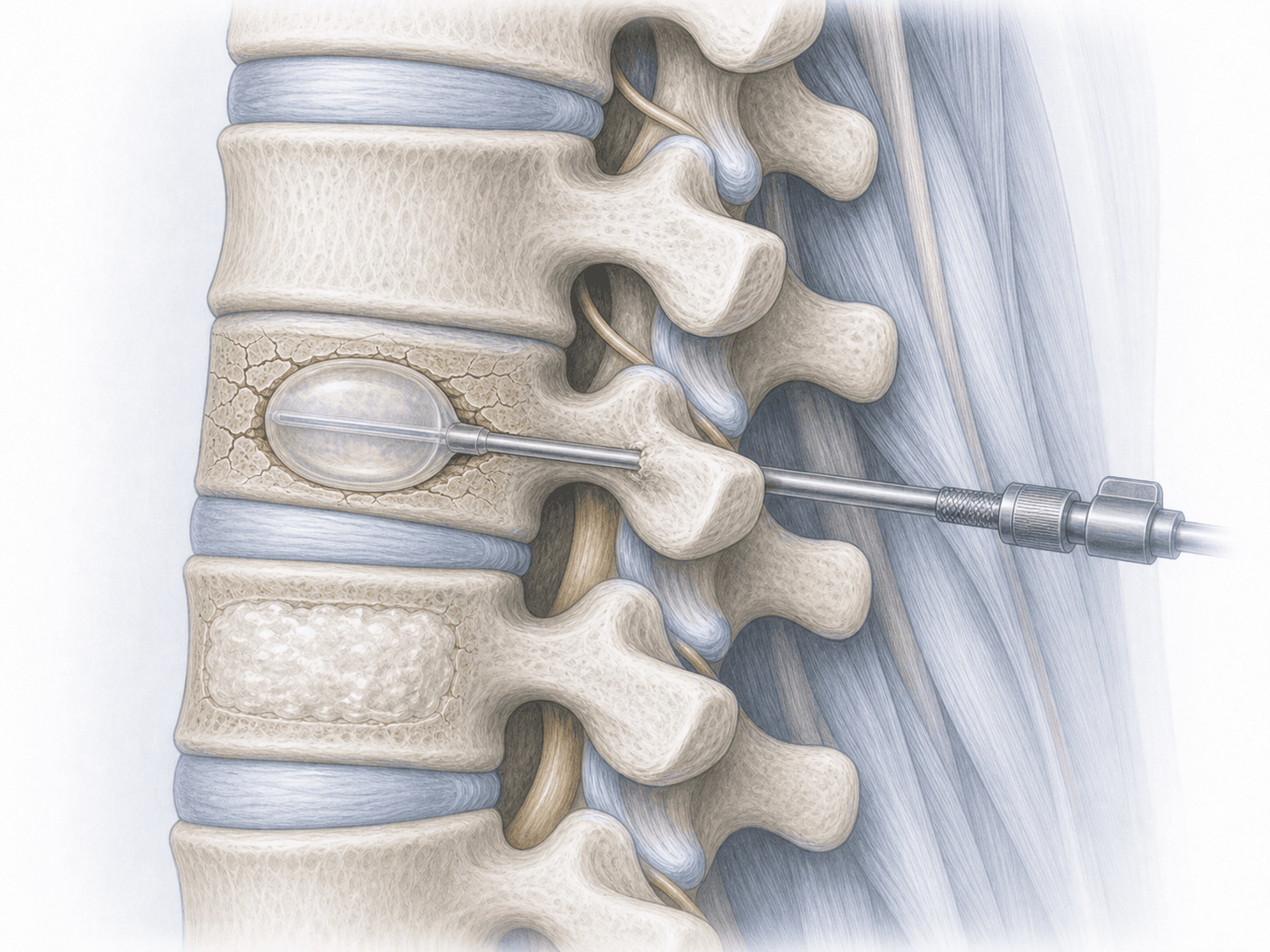
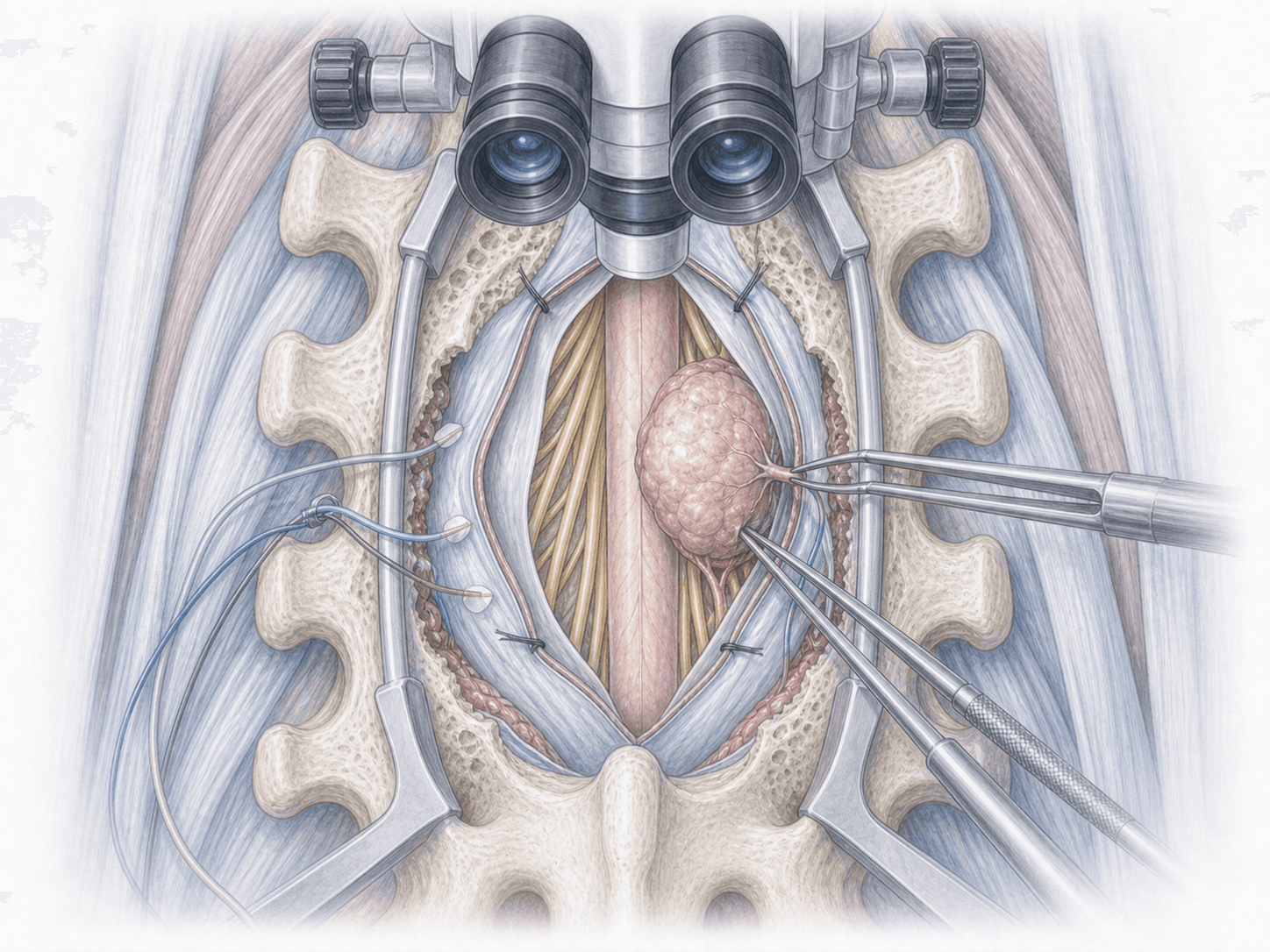
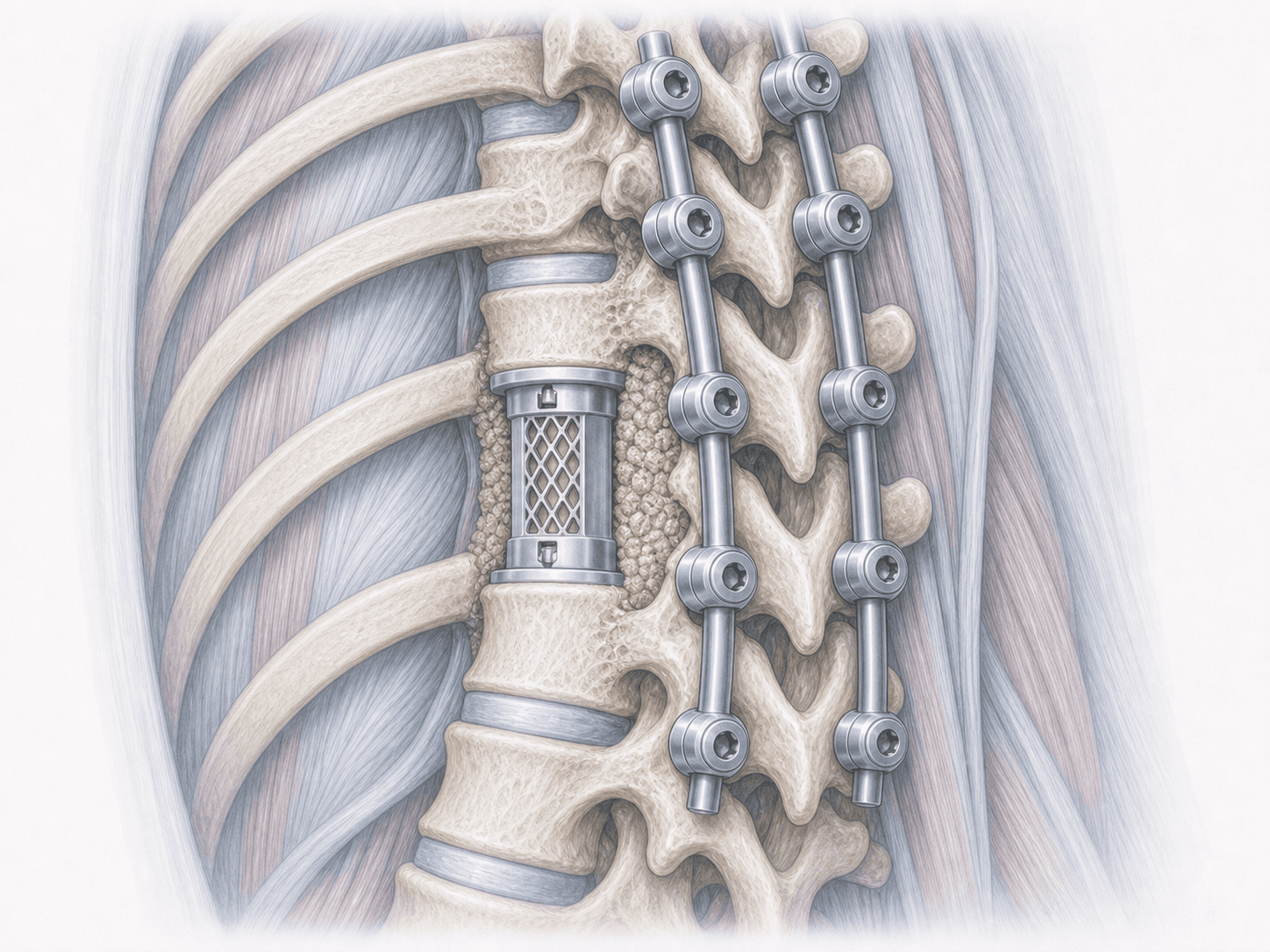
The approach is chosen according to the location and extent of the infection. In lumbar and thoracic spondylodiscitis, anterior debridement of the infected disc and vertebral bodies is usually combined with an interbody cage (titanium or PEEK with autograft) and posterior instrumentation with titanium pedicle screws to stabilise the segment. Intraoperative samples are taken for microbiology and pathology. Neurophysiological monitoring is used whenever feasible to protect neural structures.
3.Immediate postoperative period
After surgery the patient spends a few hours in recovery and is then admitted to the ward or ICU depending on the case. Targeted intravenous antibiotics are continued, with close CRP/ESR monitoring and frequent neurological checks. Mobilisation with a brace and physiotherapy start as early as the clinical situation allows. Hospital stay is usually 7–14 days, longer if needed.
Recovery after spondylodiscitis surgery
Recovery is slow and demands patience. Intravenous antibiotics are continued for several weeks and then often switched to oral treatment to complete 6 to 12 weeks in total, adjusted according to the organism and the evolution of CRP/ESR and follow-up MRI.
Light activity is resumed gradually with a brace for several weeks. Return to sedentary work is usually possible between 6 and 12 weeks; physically demanding jobs require longer. Rehabilitation, nutrition, glycaemic control and close follow-up are decisive for the final outcome. Any fever, recurrent pain or new neurological symptoms should prompt immediate review.
Risks and possible complications
Every surgery carries general risks: wound infection, bleeding, venous thrombosis or anaesthesia-related complications. In the context of spondylodiscitis there are also relevant specific risks.
The main ones are: persistent or recurrent infection despite debridement, cerebrospinal fluid leak if there are dural adhesions, nerve root or spinal cord injury (more feared at thoracic and cervical levels), instrumentation loosening or failure, pseudarthrosis or residual deformity (kyphosis) and decompensation of comorbidities such as diabetes or renal impairment due to prolonged antibiotic therapy. These risks are assessed individually and reduced through careful planning, intraoperative monitoring and close follow-up.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala