Lumbar laminotomy
Lumbar laminotomy is a less extensive decompression than a classic laminectomy. We aim to relieve pressure on the lumbar nerves by opening only the portion of the lamina needed, while preserving the spinous process, the midline ligaments and most of the bony anatomy. Many of our patients come to the clinic with neurogenic claudication: they can walk less and less before needing to stop and rest, their legs feel heavy, numb or weak, and they notice relief when they lean forward or sit down. This guide explains exactly what we do, when it is worth considering and what recovery looks like, so you can make a calm, informed decision.
What is a lumbar laminotomy?
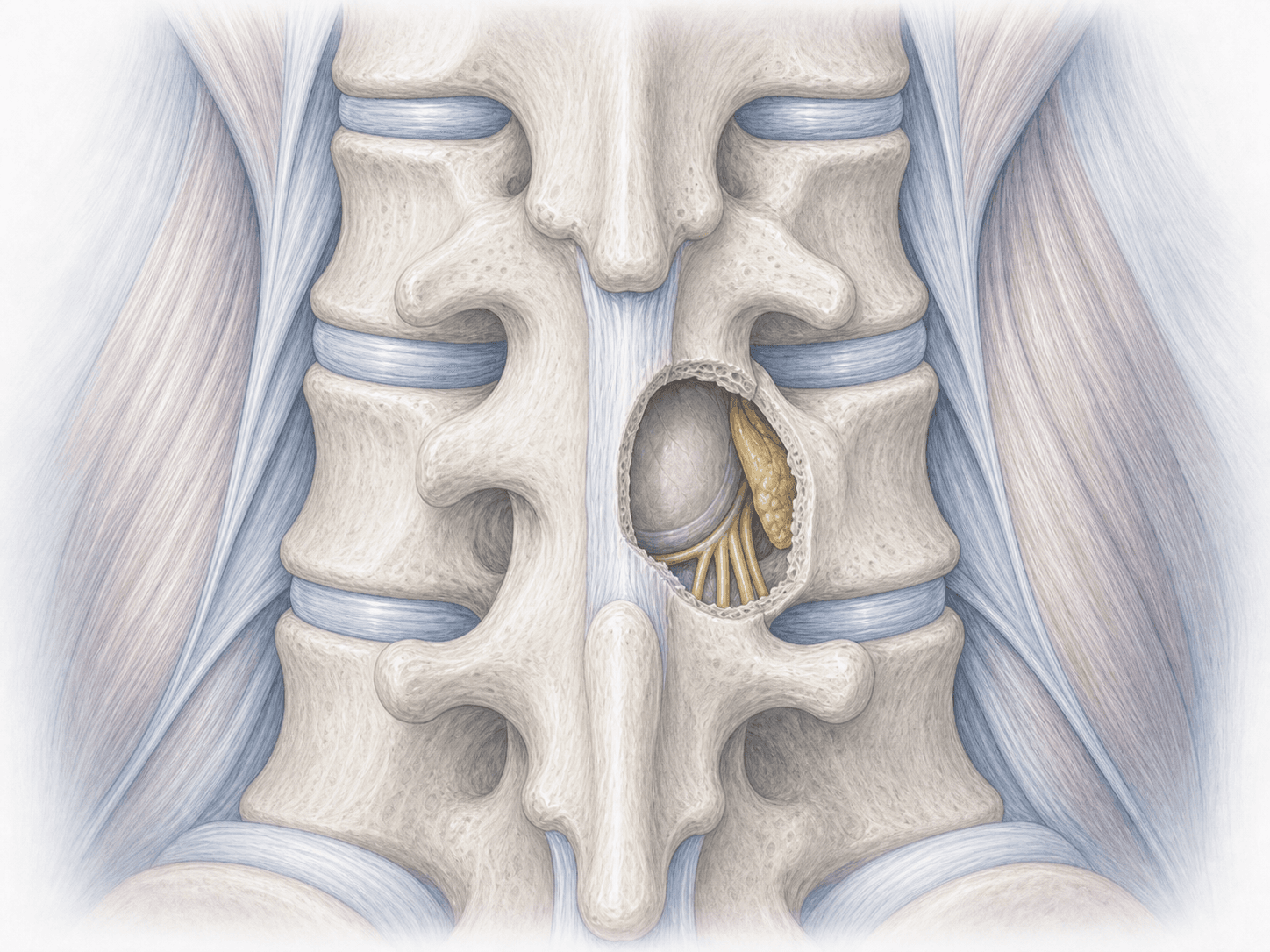
Lumbar laminotomy is a decompression technique in which we remove only part of the vertebral lamina —the bony roof of the canal— to free the nerves compressed by lumbar canal stenosis. Unlike a classic laminectomy, we do not remove the spinous process or the interspinous ligament: we respect the midline of the spine.
In many cases we can decompress both sides of the canal through a single-sided approach (unilateral approach with bilateral decompression, the so-called "over-the-top" technique). This allows us to treat central stenosis while preserving even more of the bone and muscle on the opposite side.
The main advantage over wider techniques is that, by keeping the midline stabilising structures intact, most patients do not need an added spinal fusion or a separate lateral recess decompression. If your case is a candidate, we can discuss it in detail at a personalised assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from a lumbar laminotomy usually describe a fairly recognisable pattern:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
Before surgery we review the MRI together and, if needed, dynamic flexion-extension X-rays to rule out instability. We address your concerns, walk you through exactly what we plan to do and give you the informed consent. We set fasting instructions, adjust medication (anticoagulants, anti-inflammatories) and provide tailored recommendations based on your baseline health.
2.During the procedure
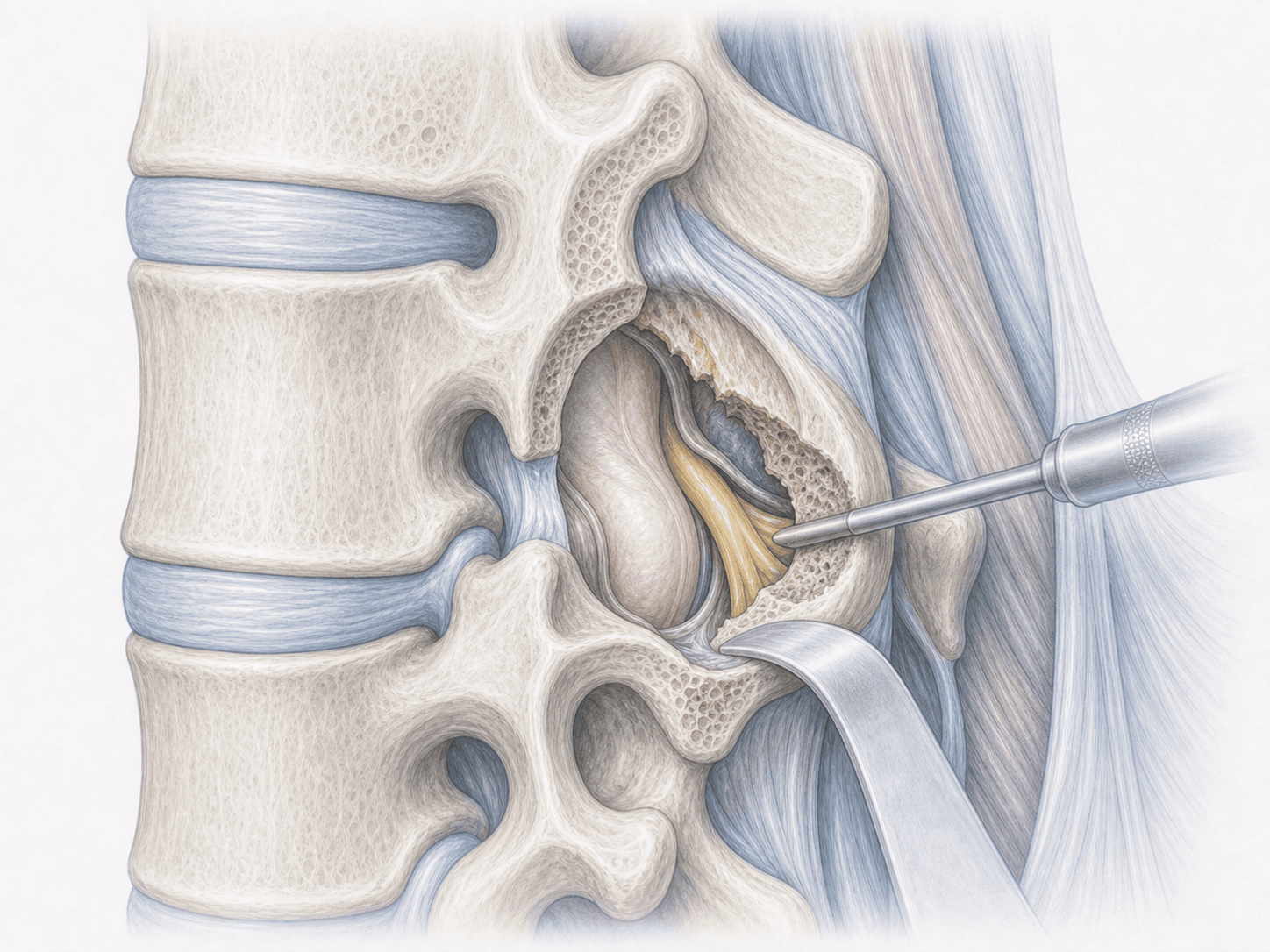
We perform the laminotomy under general anaesthesia, with you positioned prone and using the surgical microscope. We make a small midline incision and gently separate the muscle. We open a window in the lower part of the upper lamina and the upper part of the lower lamina, preserving the spinous process and the interspinous ligament.
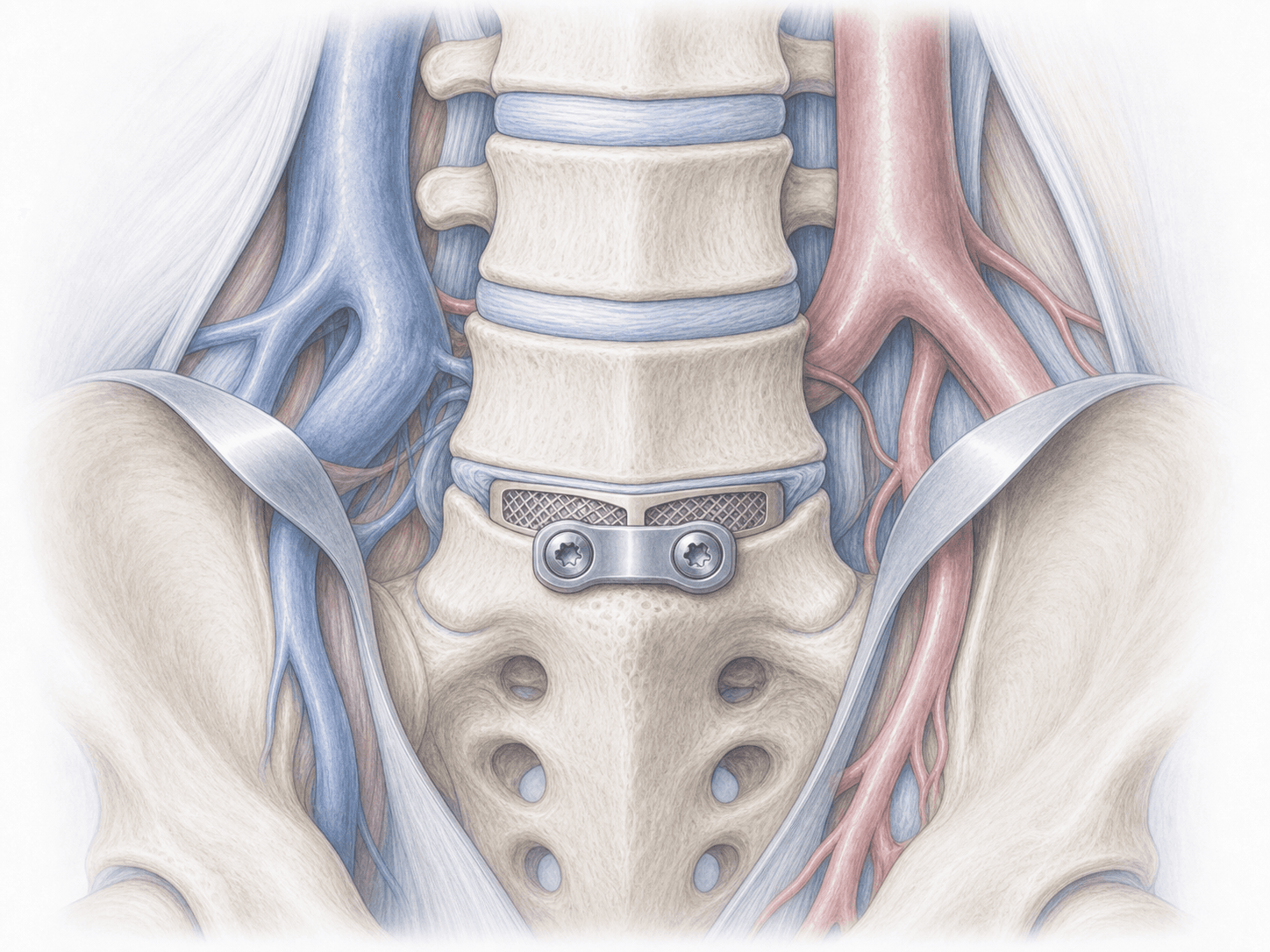
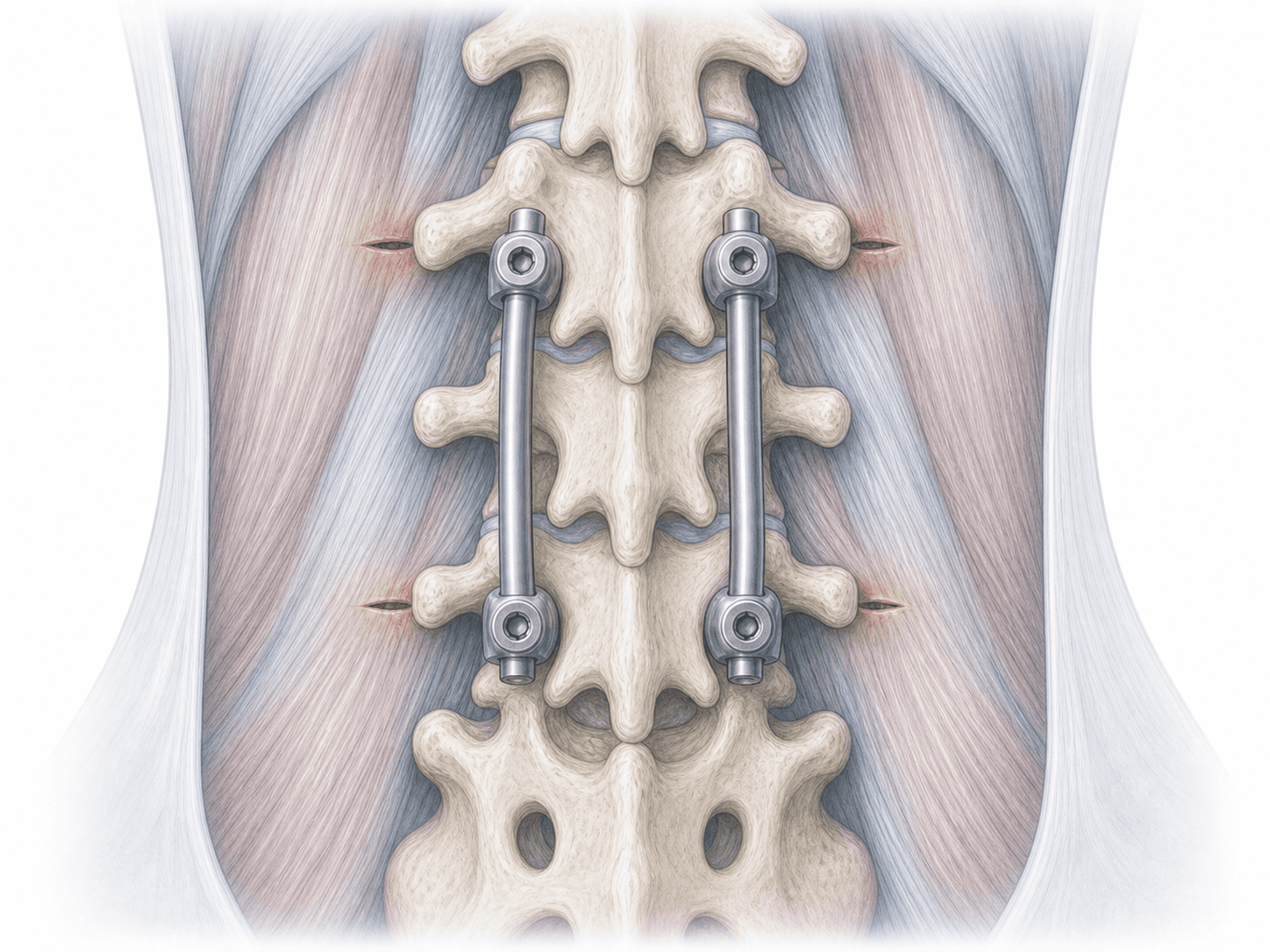
Through that window we remove the thickened ligamentum flavum and, when needed, the bone overhanging the lateral recess, decompressing the dural sac and nerve roots. When the stenosis is central and we want to preserve as much structure as possible, we tilt the table and also decompress the opposite side under the spinous process, without approaching it from outside (the "over-the-top" technique). We do not place screws or cages: no fusion.
3.Immediate postoperative period
After surgery you will spend a short time in recovery before returning to your room. We manage pain with a multimodal regimen and, as soon as analgesia allows, we help you stand up the same day or the next morning. Early walking is part of the treatment. Hospital stay is usually 24-48 hours, depending on progress and case features.
Recovery after a lumbar laminotomy
Recovery is gradual but relatively quick because no fusion is performed. Most patients walk around the house from day one, increase the distance each week and notice a clear change in their claudication within a few weeks. Leg pain relief is usually the most obvious change; background low back pain may take a little longer to settle.
Office work is typically resumed in 2 to 4 weeks. Physical or heavy work requires more time and a gradual return, usually 6 to 12 weeks. We recommend avoiding heavy lifting and abrupt bending in the early weeks, and as soon as we clear you we start a rehabilitation programme focused on lumbar stability and walking. If you develop fever, disproportionate pain, new weakness or urinary problems, you should contact us straight away.
Risks and possible complications
Every surgery involves general risks such as infection, bleeding, thrombosis or anaesthesia-related issues.
Specific risks of lumbar laminotomy include a dural tear with cerebrospinal fluid leak (which we usually repair during the same operation), nerve root injury, incomplete decompression with persistent symptoms, mid- or long-term recurrence of stenosis, or postoperative instability that may, in a small percentage of cases, require a later fusion. We assess these risks individually and explain them in detail before deciding.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala