Transforaminal epidural injections
A transforaminal epidural injection is a minimally invasive procedure that targets radicular pain — typical sciatica or cervicobrachial pain — by delivering corticosteroid right next to the inflamed nerve root, reaching it through the neural foramen under image guidance. Many patients consider it when leg or arm pain does not improve with rest, physiotherapy or medication, but they do not want — or do not yet need — surgery. This guide explains when it is indicated, how it is performed step by step and what to realistically expect in the days and weeks afterwards.
What is a transforaminal epidural injection?
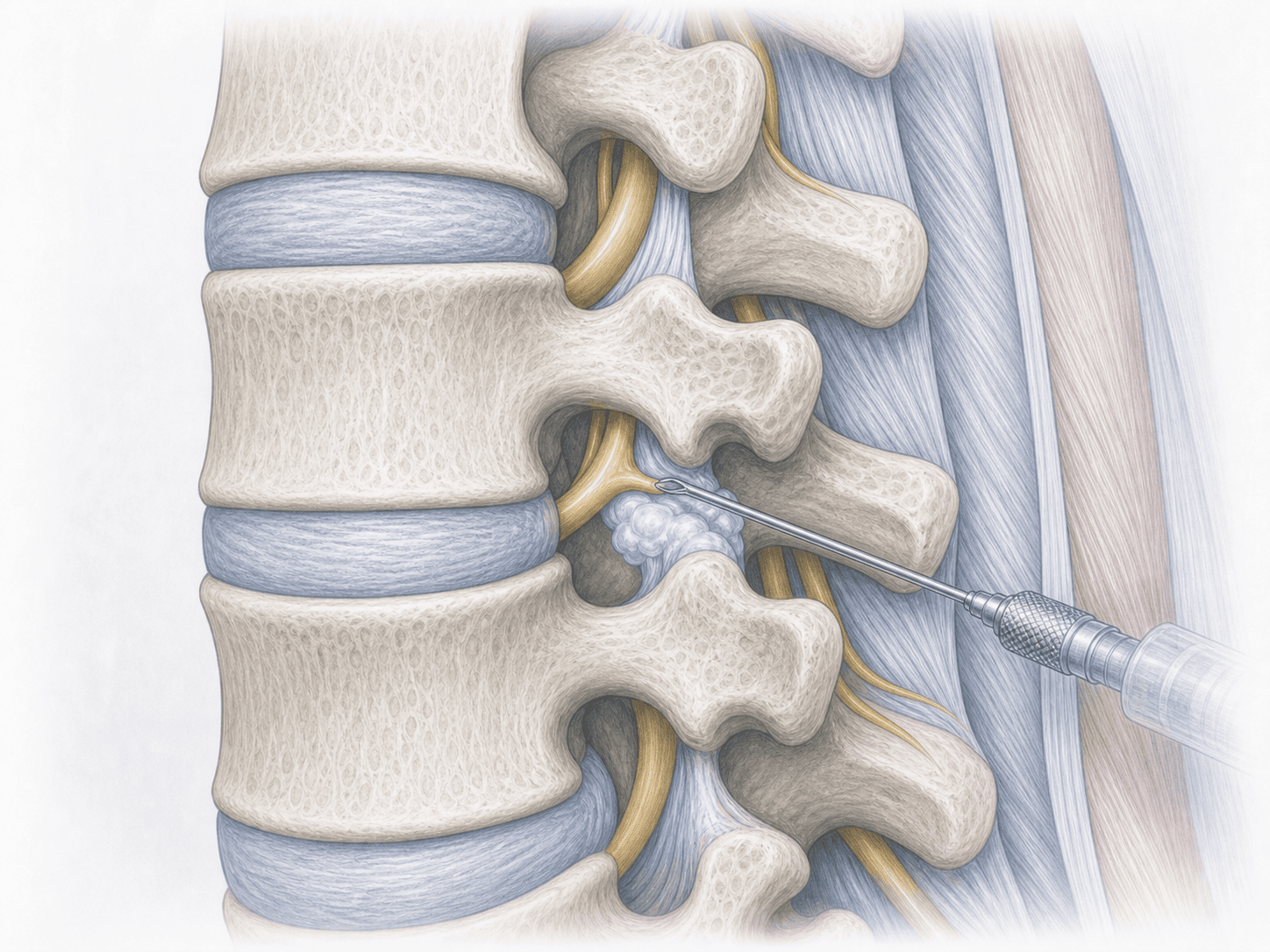
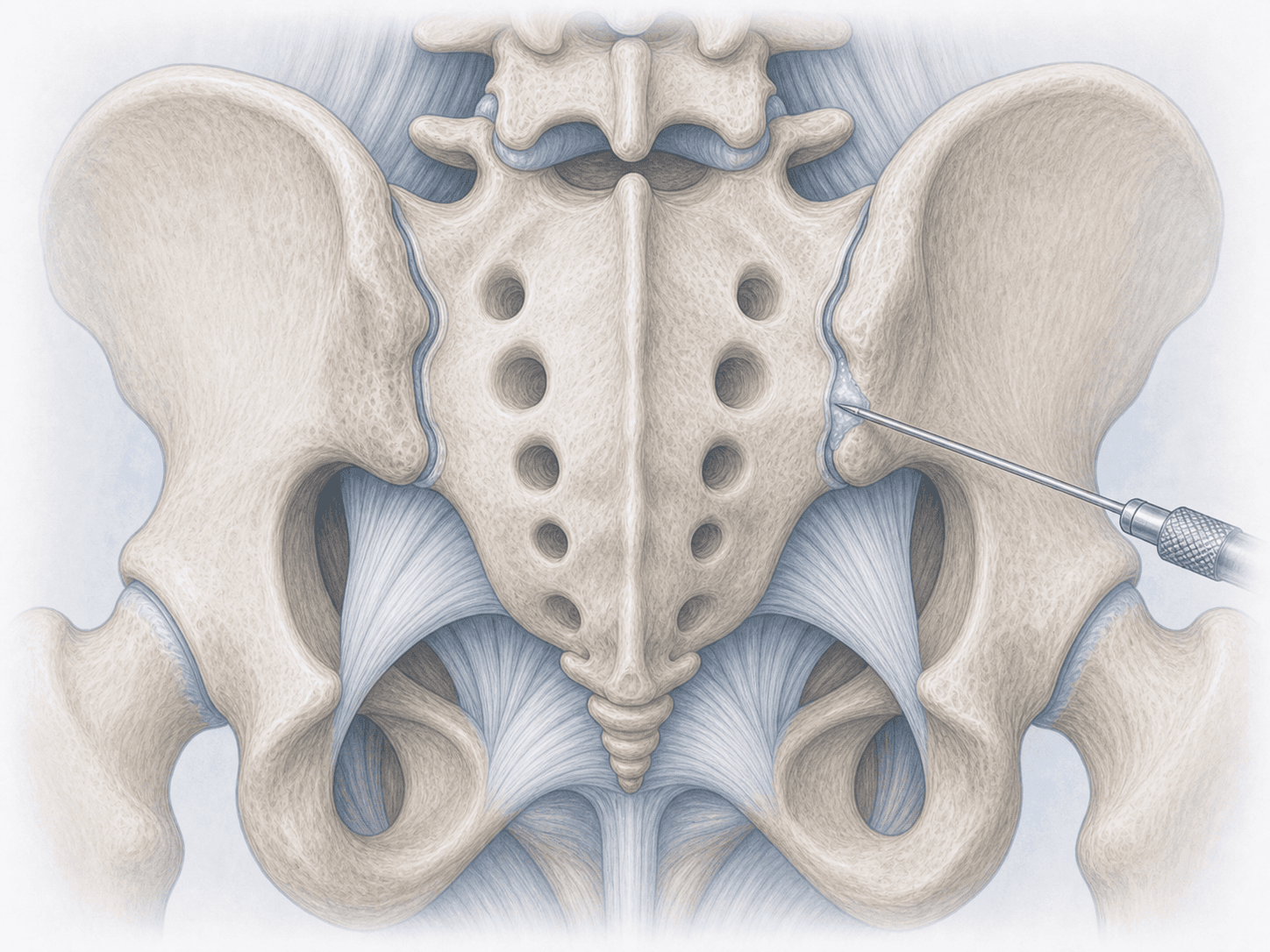
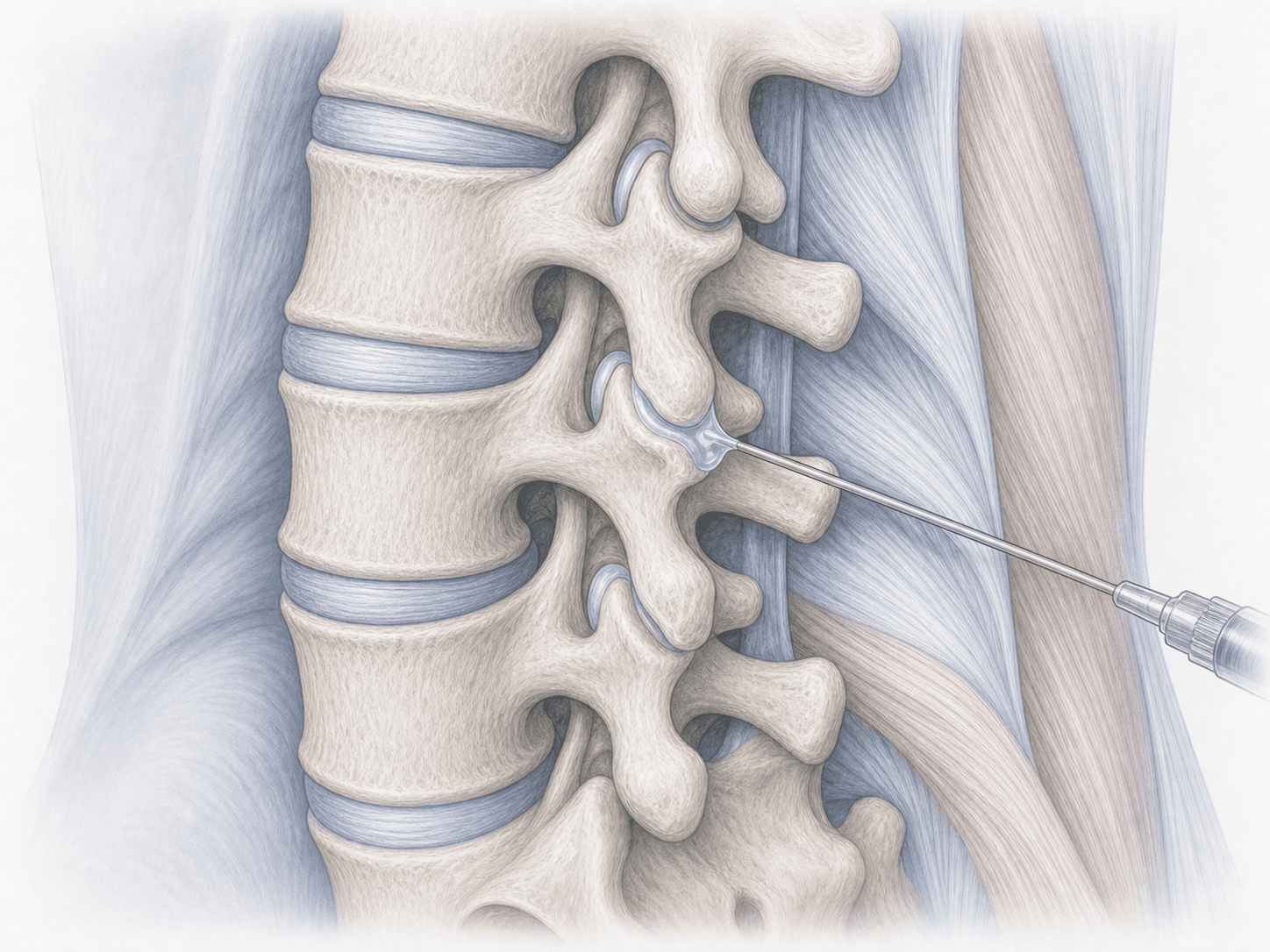
A transforaminal epidural steroid injection (TFESI) is a pain-intervention technique in which, under fluoroscopic guidance and using iodinated contrast, a thin needle is advanced through the neural foramen — the opening where each nerve root exits the spine — until its tip sits in the anterior epidural space, right next to the symptomatic nerve root. A mixture of corticosteroid and local anaesthetic is then deposited there to reduce perineural inflammation.
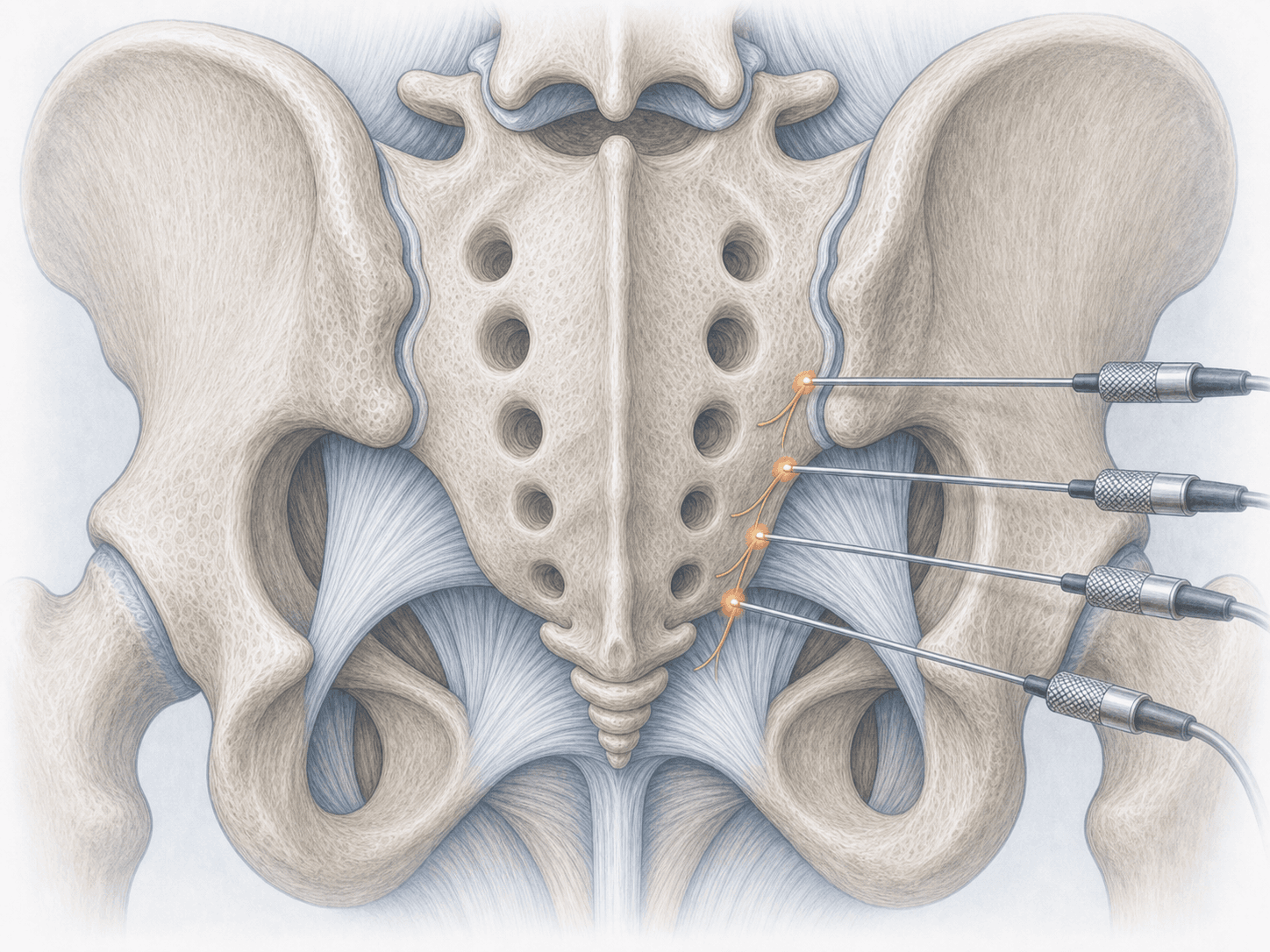
Unlike a classic interlaminar epidural, which bathes several roots at once, the transforaminal route is selective: it targets the specific root producing symptoms. That is why it is used when there is a clear match between imaging (a disc herniation or foraminal stenosis at one level) and the pain pattern described by the patient.
It is an outpatient procedure. Non-particulate corticosteroids are used in the cervical spine for vascular safety, and whenever possible the injection is offered as a therapeutic bridge to avoid or delay more aggressive surgery such as lumbar microdiscectomy. If radicular pain is limiting your daily life, you can request an assessment with Dr. Ben Ghezala to review your MRI and decide whether the injection is a reasonable option in your case.
Symptoms and warning signs
Patients who may benefit from a transforaminal injection usually describe:
When is a transforaminal injection indicated?
How is the procedure performed?
1.Preoperative preparation
The MRI and clinical history are reviewed to confirm the target root and level. It is essential to disclose anticoagulant or antiplatelet use, iodinated contrast allergies and any active infection. Strict fasting is usually not required when only local anaesthesia is used, although exact instructions are given during the preoperative visit.
2.During the procedure
The patient lies prone for lumbar approaches or supine with slight head rotation for cervical levels. After skin antisepsis and local anaesthesia, the needle is advanced under fluoroscopy to the foramen of the target root. A small amount of iodinated contrast is injected and real-time imaging confirms an epidural and perineural pattern — not vascular. Once the position is verified, the corticosteroid and local anaesthetic mixture is delivered. The whole procedure typically lasts 15–30 minutes.
3.Immediate postoperative period
The patient is observed for 20–30 minutes to monitor blood pressure, sensation and strength in the limb. Mild numbness in the area for a few hours due to the local anaesthetic is common. Driving the same day is not advised and light activity is recommended. Most patients go home on their own without admission.
Recovery after a transforaminal injection
The first 24–48 hours may bring a mild flare of pain (rebound effect) before the corticosteroid starts to work. Relief usually begins between day 3 and day 7 and consolidates over 2–3 weeks. How long the benefit lasts varies a lot: weeks in some patients, months in others, depending on the underlying cause and how much the inflammation settles.
It is a good time to resume physiotherapy and the prescribed exercise plan, because the pain-free window allows real work on muscle strength and posture. If the pain returns, the injection can be repeated (usually no more than 3–4 per year at the same level) or the plan can be reassessed, including the surgical option when indication justifies it.
Risks and possible complications
Transforaminal injection is a safe procedure when performed by an experienced operator under image guidance, but it is not risk-free.
The most common effects are mild: transient pain at the puncture site, facial warmth for 24–48 hours, a brief glucose rise in diabetic patients or short-lived insomnia from the corticosteroid. Uncommon risks include dural puncture with postdural-puncture headache, epidural haematoma, local infection or contrast reaction. In cervical injections, non-particulate corticosteroids are used to minimise the very rare risk of vascular embolism from accidental injection into a radicular artery. These points are weighed on a case-by-case basis before recommending the procedure.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala