Thoracic discectomy
Thoracic discectomy is a technically demanding operation that we only consider when a disc herniation in the dorsal spine is causing band-like radiating pain, leg weakness or signs of myelopathy. Symptomatic thoracic herniations are uncommon (around 1% of all herniations requiring surgery) and many are central or calcified, so the surgical approach makes a real difference in the neurological outcome. This guide explains when it is indicated, which approaches we use —posterolateral or anterior/transthoracic— and what to expect from recovery, with an honest message about the complexity of this type of surgery.
What is thoracic discectomy?
Thoracic discectomy is the surgery that removes a herniated disc fragment in the dorsal spine (between T1 and T12) that is compressing the spinal cord or a nerve root. Unlike the cervical or lumbar spine, the thoracic canal is narrow and the spinal cord has little margin, so any surgical approach must avoid manipulating it.
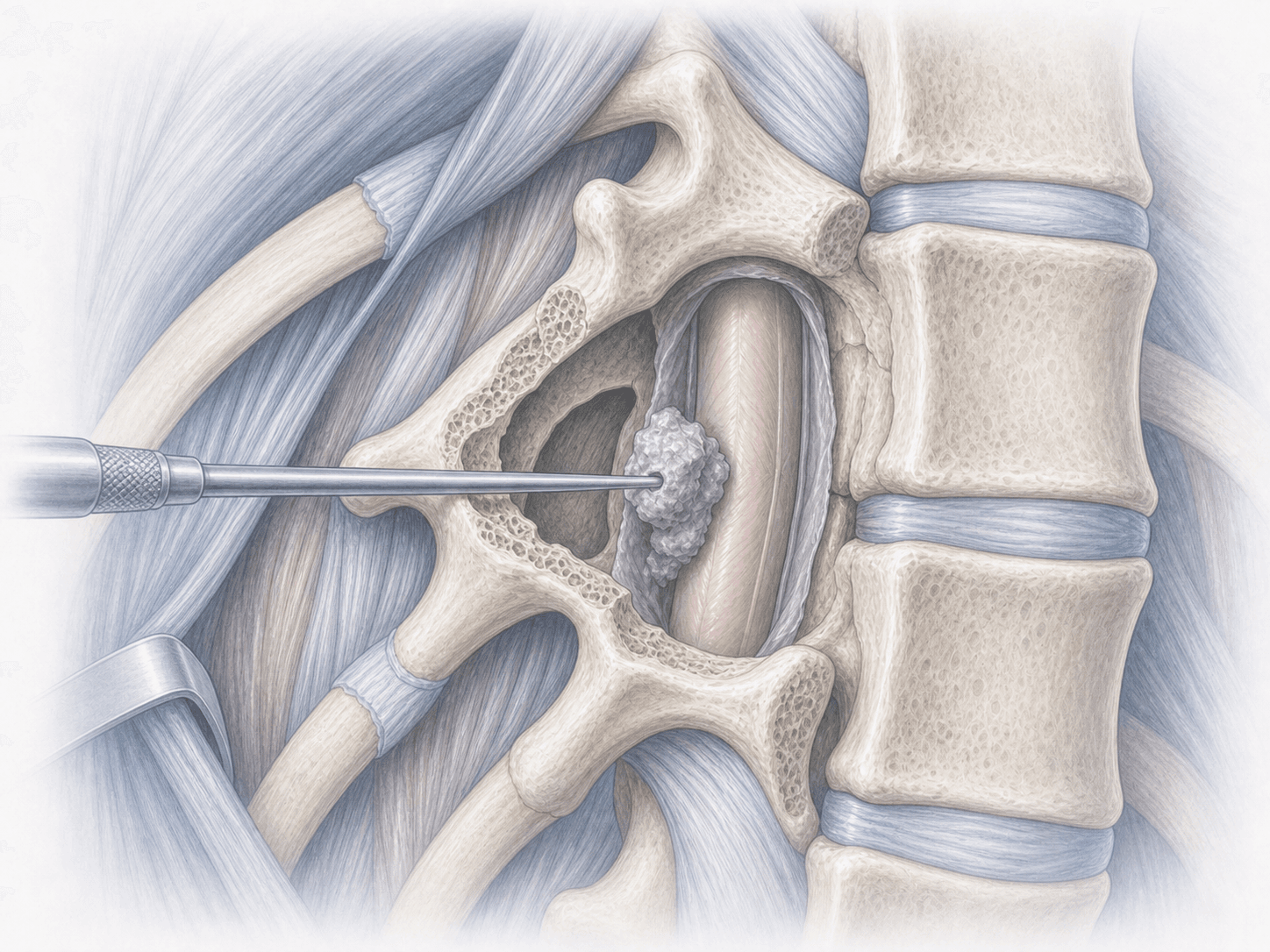
We use approaches designed to reach the disc without crossing the spinal cord: a posterolateral route (transpedicular, costotransversectomy or retropleural) for lateral or soft herniations, and an anterior approach via thoracotomy or mini-thoracotomy for central, calcified or strongly adherent herniations. Classical laminectomy is almost always avoided because it requires mobilising the cord and carries a high risk of postoperative myelopathy.
When the hernia is small, soft and lateral, a minimally invasive thoracic microdiscectomy may be appropriate. To discuss your specific case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients with a symptomatic thoracic disc herniation often describe a mixed clinical picture, combining mid-back pain with chest, abdominal or leg symptoms:
When is this surgery indicated?
How is the procedure performed?
1.Preoperative preparation
Before surgery we review MRI, CT and, if needed, CT myelography to localise the level precisely and characterise the herniation (soft, calcified, central or lateral). The target segment is confirmed with preoperative radiological marking and, depending on the approach, pulmonary function is assessed for transthoracic routes. You will receive fasting instructions, medication adjustments (anticoagulants, antiplatelets) and tailored recommendations.
2.During the procedure
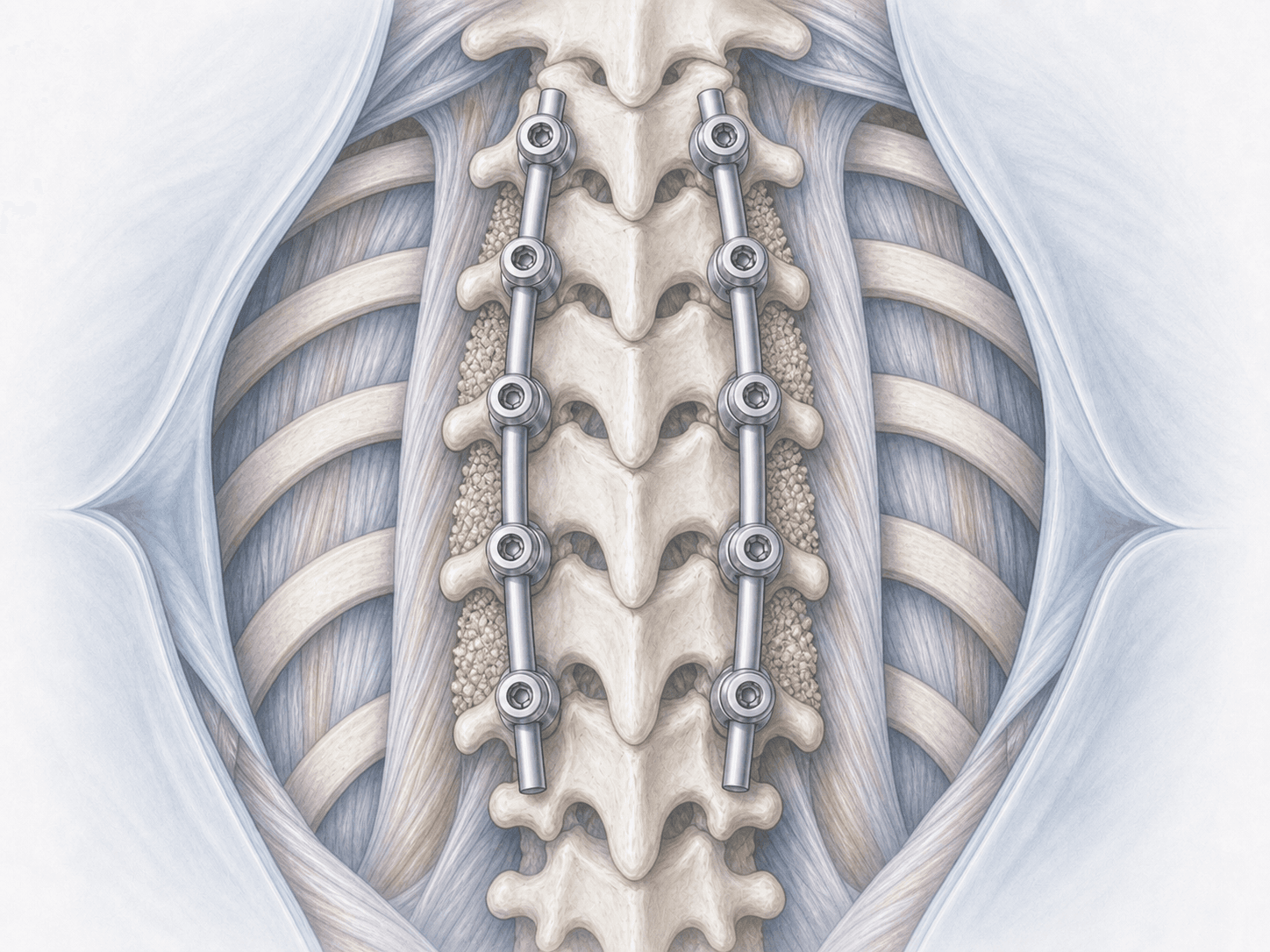
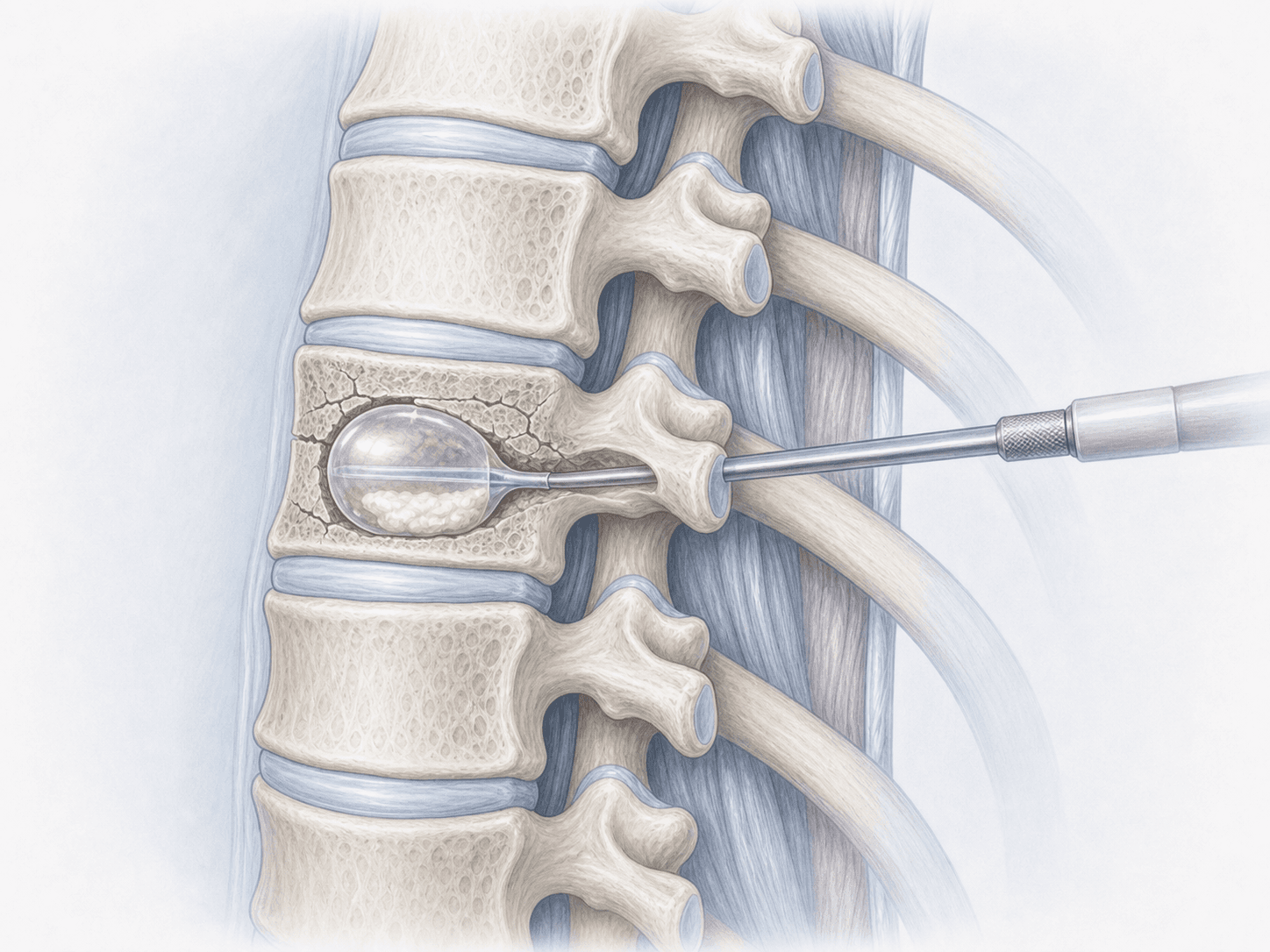
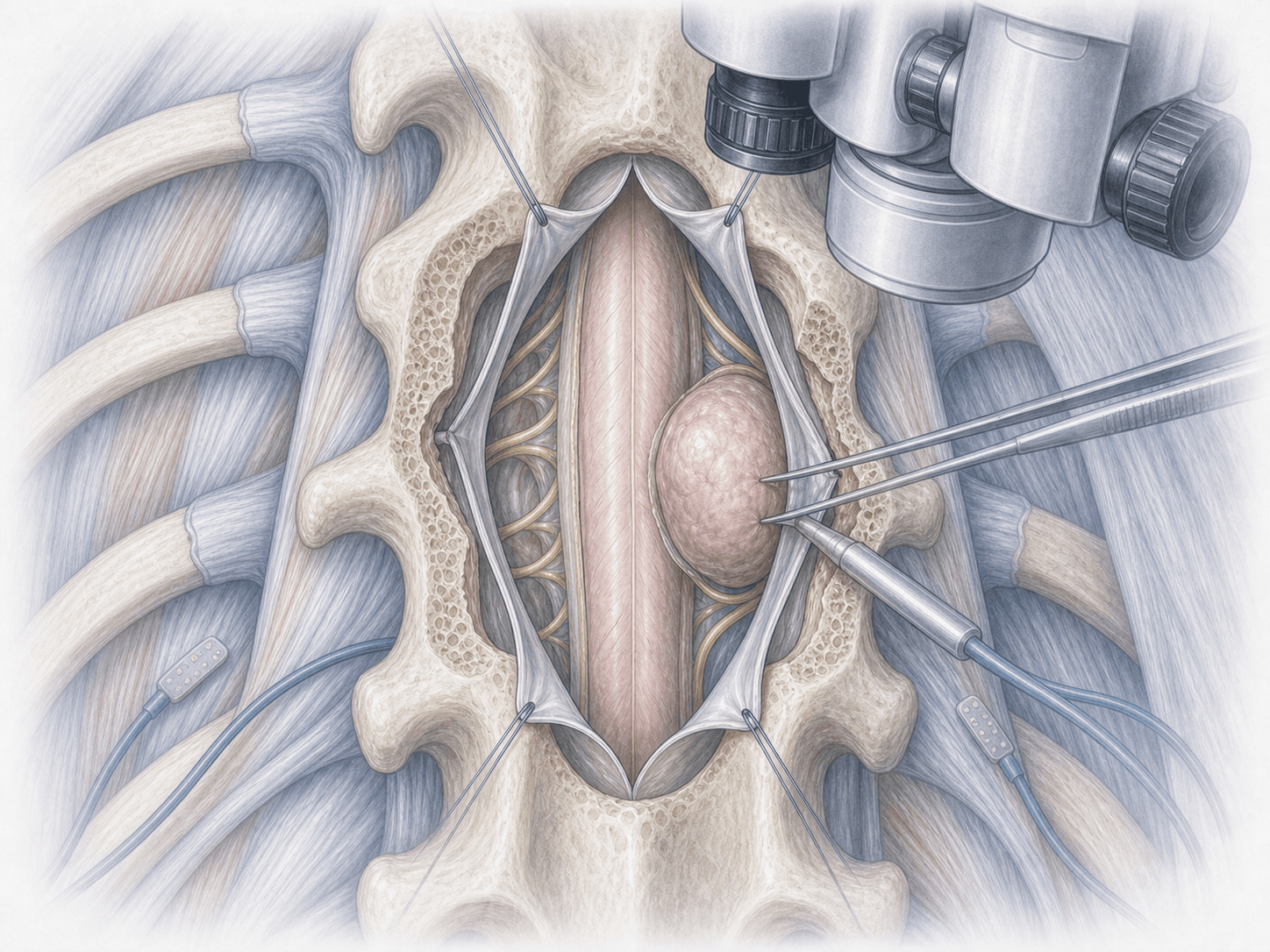
Surgery is performed under general anaesthesia with intraoperative neurophysiological monitoring (motor and somatosensory evoked potentials) to track spinal cord function in real time. We choose the approach according to the hernia's location and consistency. For lateral or soft herniations we use a posterolateral approach (transpedicular, costotransversectomy or retropleural) and reach the disc around the cord without retracting it. For central, calcified or strongly adherent herniations we reserve an anterior approach via thoracotomy or mini-thoracotomy, which allows removal under direct vision and minimises spinal cord handling. After removing the herniated fragment we reconstruct the defect with the appropriate material and, if resection compromises stability, we add instrumentation.
3.Immediate postoperative period
After surgery you will spend several hours in recovery with close neurological monitoring. Transthoracic approaches usually require a pleural drain for 24–72 hours. Gradual mobilisation begins on day 1 or 2 depending on the approach. Hospital stay is typically 3–6 days, longer than in cervical or lumbar surgery because of the complexity of the access.
Recovery after thoracic discectomy
Recovery after thoracic discectomy is slower than after other spine procedures and depends heavily on the approach. The first 2–4 weeks focus on wound care, pain control and, in anterior approaches, recovery of respiratory mechanics.
Return to a sedentary job typically occurs between 4 and 8 weeks. For physical jobs or those with significant respiratory load, timelines extend to 3 months or more. Specific rehabilitation —respiratory in thoracic approaches, postural and core strengthening— is part of the plan from the early weeks.
Neurological recovery depends on how long the cord was compressed: the earlier we act on myelopathy, the higher the chance of improvement. Any fever, breathing difficulty, disproportionate pain or new neurological deficit should be reported promptly.
Risks and possible complications
Thoracic discectomy carries a higher risk profile than cervical or lumbar surgery, which is why we only indicate it when the expected neurological benefit is clear.
In addition to the general surgical risks (infection, bleeding, thrombosis, anaesthesia-related issues), there are specific risks: spinal cord injury with paraparesis or paraplegia, nerve root injury, cerebrospinal fluid leak, pneumothorax or pleural effusion in transthoracic approaches, postoperative intercostal neuralgia, residual herniation and, less commonly, the need for subsequent instrumentation due to instability. Each case is assessed individually to choose the approach that minimises risk for your specific anatomy.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala