Lumbar microdiscectomy
Lumbar microdiscectomy is a minimally invasive operation that removes the disc herniation fragment compressing a lumbar nerve root, most often at L4-L5 or L5-S1. Many patients reach the clinic after weeks or months of severe sciatica, leg tingling or weakness that does not improve with rest, physiotherapy, medication or injections. This guide explains realistically how the procedure is performed, what to expect during recovery and when it is indicated, so you can decide calmly and with full information.
What is lumbar microdiscectomy?
Lumbar microdiscectomy is a surgical procedure that removes the disc herniation fragment compressing a nerve root in the lumbar spine, usually at L4-L5 or L5-S1. We work under a surgical microscope through a small incision and, in most cases, with a tubular retractor that separates the muscle without cutting it.
Compared with alternatives such as endoscopic lumbar discectomy, microdiscectomy offers a wide microscopic view and direct control of the nerve root, especially useful in extruded or migrated herniations. To assess your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from lumbar microdiscectomy typically report:
When is lumbar microdiscectomy indicated?
How is the procedure performed?
1.Preoperative preparation
It includes a clinical assessment, review of the MRI and discussion of any concerns. You will receive fasting instructions, medication adjustments (anticoagulants, antiplatelets) and tailored recommendations based on your case and comorbidities.
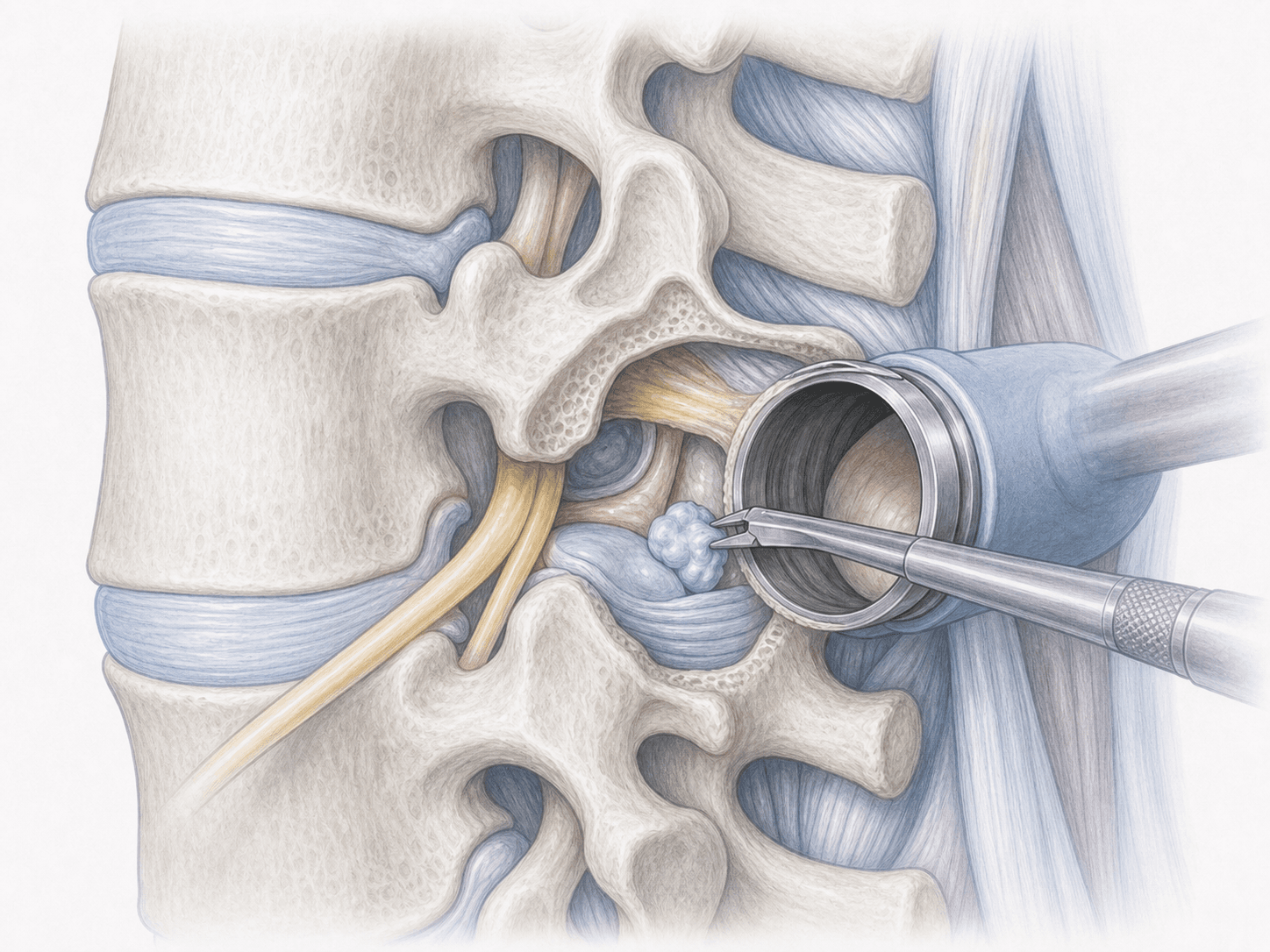
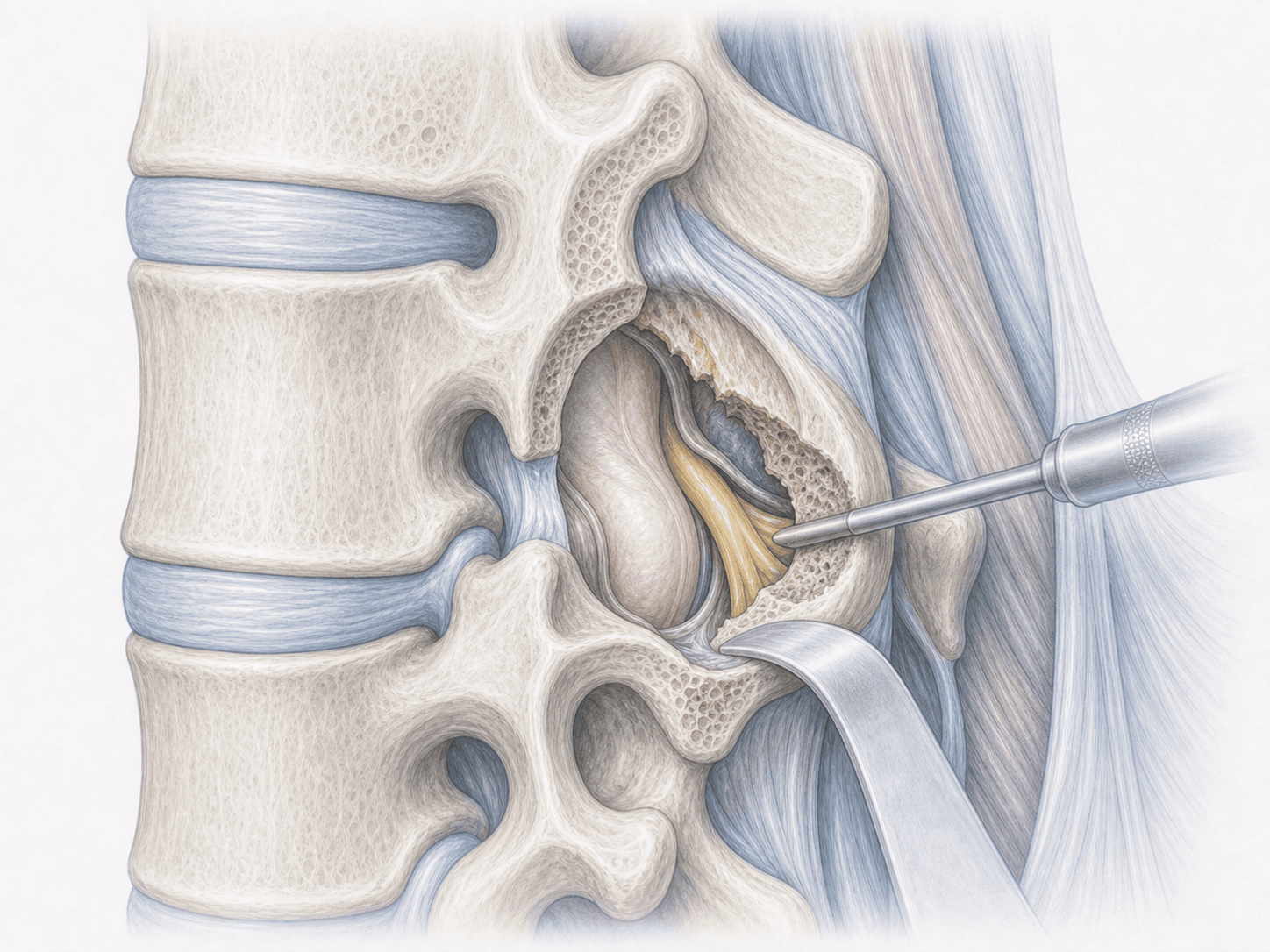
2.During the procedure
We operate under general anaesthesia with the patient in the prone position. We locate the affected level with fluoroscopy and make an incision of about 2-3 centimetres. A tubular retractor separates the muscle without cutting it and we work under the microscope. We remove only the necessary ligamentum flavum, identify the nerve root and extract the herniated fragment compressing it, preserving as much disc and segmental stability as possible.
3.Immediate postoperative period
After surgery, patients spend a short time in recovery before returning to their room. Mobilisation starts the same day or the following morning, with progressive sitting and walking. Hospital stay is usually 24 hours, except in selected cases that require a longer stay due to comorbidities or clinical safety.
Recovery after lumbar microdiscectomy
Sciatica relief is usually noticeable soon after surgery, sometimes on waking up. Mild low back pain at the incision improves within a few days with standard analgesia.
We return to daily life gradually: walking every day from the start and avoiding heavy lifting, sudden twists and long periods of sitting during the first weeks. Office work is usually resumed within 2-4 weeks; physical or lifting jobs between 6 and 8 weeks. Guided physiotherapy typically starts at 3-4 weeks. Fever, increasing low back pain, new weakness or bowel or bladder changes warrant prompt medical review.
Risks and possible complications
All surgery carries general risks such as infection, bleeding, thrombosis or anaesthesia-related complications.
Specific risks of lumbar microdiscectomy include nerve root injury (uncommon), cerebrospinal fluid leak from a dural tear, recurrent herniation at the same level (around 5-10 per cent in published series), residual low back pain and, exceptionally, disc space infection (spondylodiscitis). These risks are assessed individually for each patient.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala