Thoracic laminectomy
Thoracic laminectomy is an operation that removes the back portion of one or several thoracic vertebrae (the laminae) to release the spinal cord when it is compressed by severe stenosis, a hypertrophied or ossified ligamentum flavum, or extradural tumours. Many patients reach this stage after noticing balance problems, progressive leg weakness or a band-like mid-back pain that no longer improves with conservative treatment. In this guide we explain in plain language when it is indicated, how we plan it, what to expect during recovery and which decisions we take together so you understand every step before going to theatre.
What is thoracic laminectomy?
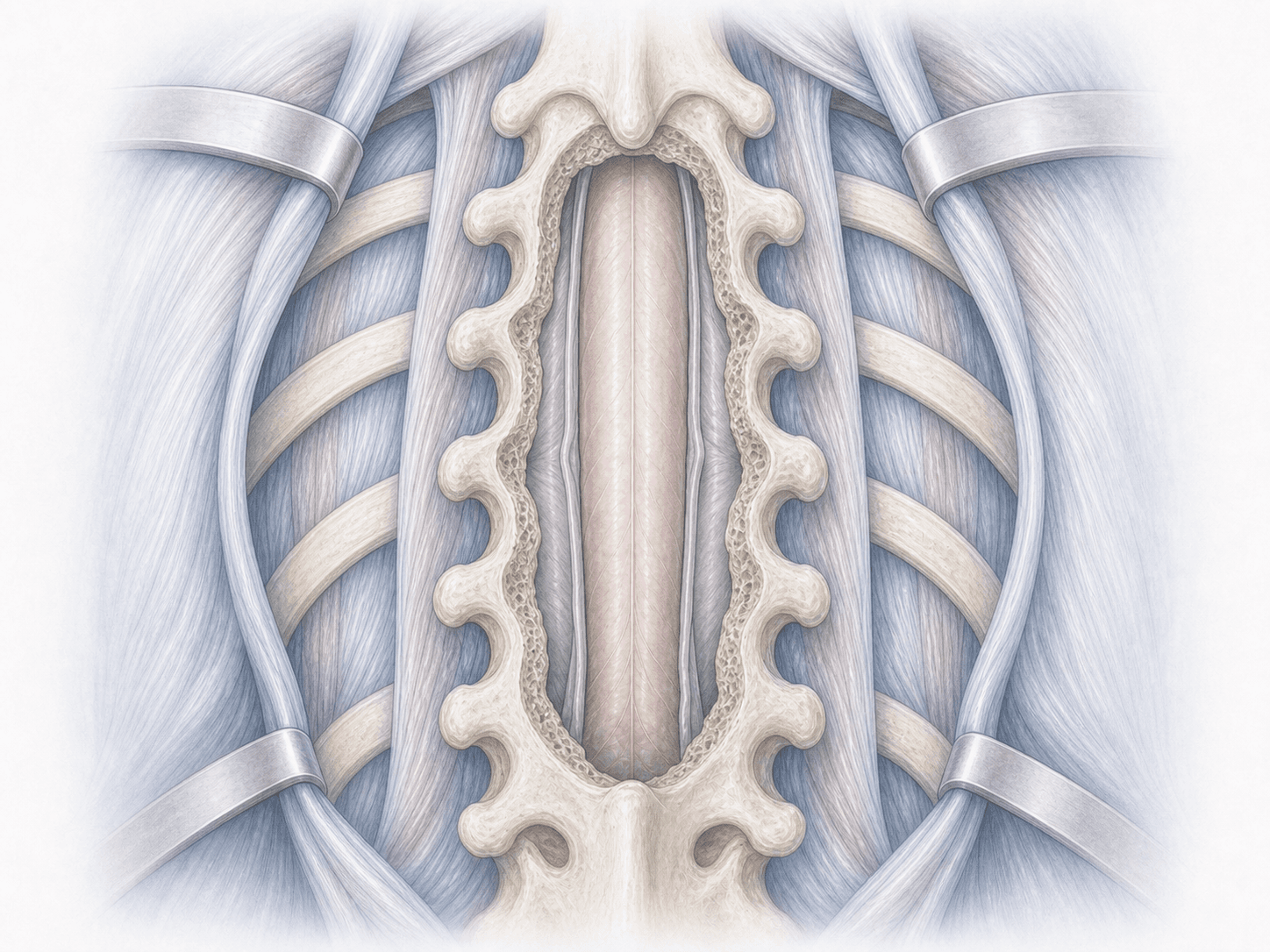
Thoracic laminectomy is a decompressive operation performed through a posterior approach. We remove the laminae (the bony roof of the thoracic vertebrae) to free the spinal cord and, when needed, part of the thickened or ossified ligamentum flavum that is compressing it.
Unlike the cervical or lumbar spine, the thoracic cord sits in a narrow canal with a more vulnerable blood supply, so any decompression requires careful planning and continuous intraoperative neurophysiological monitoring. Laminectomy is one of the cornerstones of surgical treatment for thoracic spinal canal stenosis, and in selected cases it is completed with an instrumented fusion when several levels are removed. To discuss your specific case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from a thoracic laminectomy typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
Before surgery we review your MRI and CT together to pinpoint the compressed level (the thoracic spine is tricky because the ribs make intraoperative counting difficult). We arrange blood tests, cardiopulmonary assessment and, in patients on anticoagulants, plan how to pause them safely. We explain the procedure, answer your questions and give you instructions about fasting, medication adjustments and skin preparation.
2.During the procedure
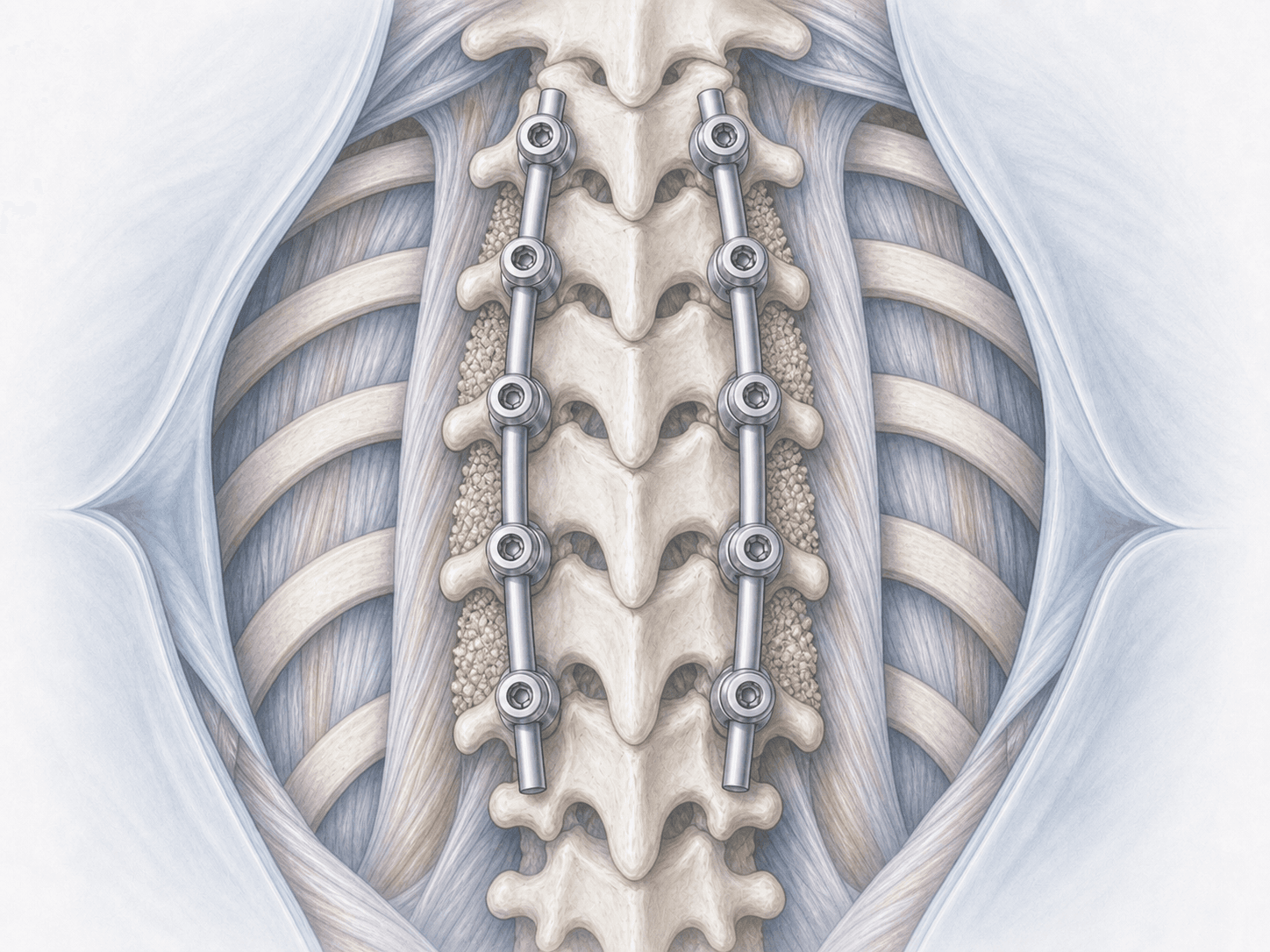
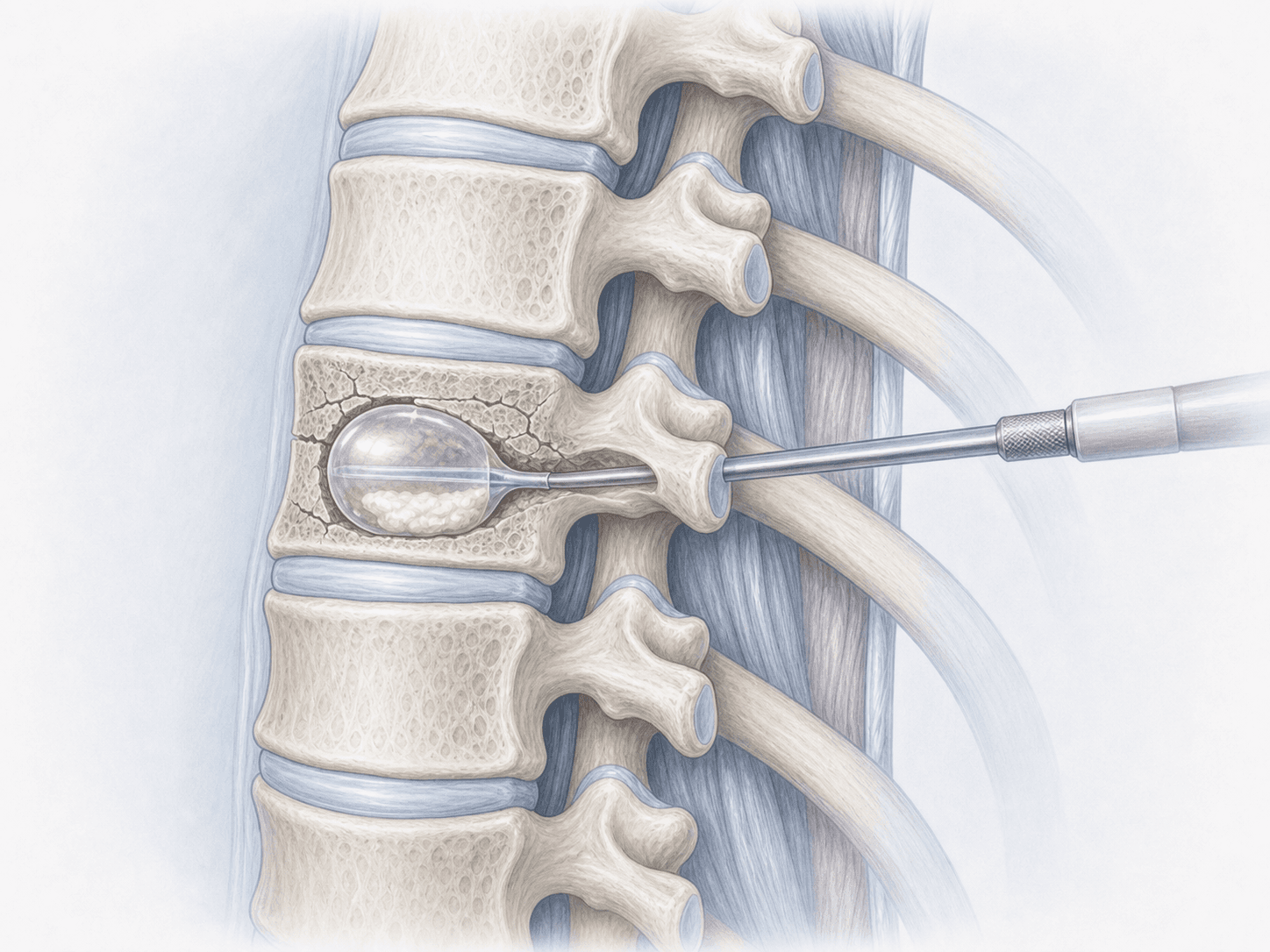
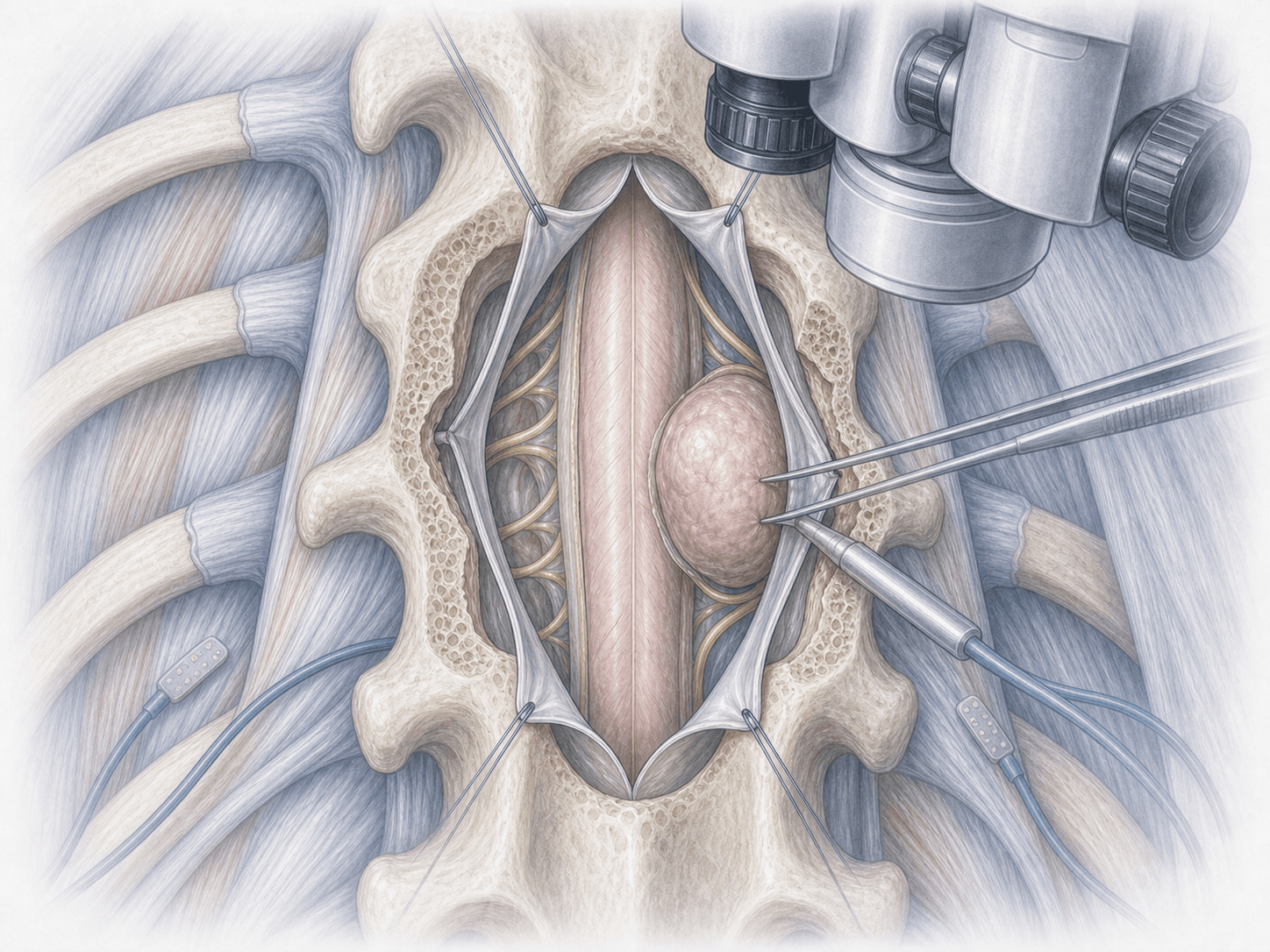
We operate under general anaesthesia, in prone position and with continuous neurophysiological monitoring (motor and somatosensory evoked potentials), which we consider mandatory in thoracic surgery. We confirm the level with fluoroscopy, make a midline posterior incision and remove the laminae and the ligamentum flavum either en bloc or piecemeal, always keeping the spinal cord under direct vision. When the decompression spans several levels or there is a risk of post-laminectomy kyphosis, we add pedicle screws and rods to stabilise the segment.
3.Immediate postoperative period
You spend a few hours in recovery while we monitor your neurological exam, pain control and drain. We usually get you out of bed the next day with physiotherapy support. Hospital stay is typically 3 to 5 days, somewhat longer if an instrumented fusion was added or in patients with significant comorbidities.
Recovery after thoracic laminectomy
Recovery is gradual. During the first 2–4 weeks we focus on walking, postural hygiene and gradual control of the incision pain. Sedentary activities are usually resumed between weeks 3 and 6, while physical jobs require 2–3 months, longer if a fusion was added.
Neurological recovery depends a lot on how long the cord was compressed and how severe the myelopathy was: band-like pain often improves quickly, while strength and balance recover over months with rehabilitation. Fever, severe pain, wound fluid leak or new neurological symptoms warrant immediate review.
Risks and possible complications
All surgery carries general risks such as infection, bleeding, thrombosis or anaesthesia-related issues.
Specific risks of thoracic laminectomy include spinal cord or root injury (uncommon, and the reason why we use continuous monitoring), cerebrospinal fluid leak from a dural tear, transient or permanent neurological deficit, postoperative epidural haematoma and, in the medium term, kyphotic deformity when several levels are decompressed without fusion. That is why we assess in every case whether instrumentation should be added.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala