Thoracic microdiscectomy
Thoracic microdiscectomy is the minimally invasive version of dorsal disc herniation surgery: we use the operating microscope and a posterolateral approach (transpedicular or facet-sparing transfacet) to remove the herniation through a small incision. It is the option we consider when the herniation is soft and lateral or paramedian, and we want to avoid both anterior transthoracic approaches and instrumented fusion. For markedly calcified, central herniations the approach may need to be different and we discuss it on a case-by-case basis. This guide explains when it is indicated, how we perform it step by step and what recovery to expect.
What is thoracic microdiscectomy?
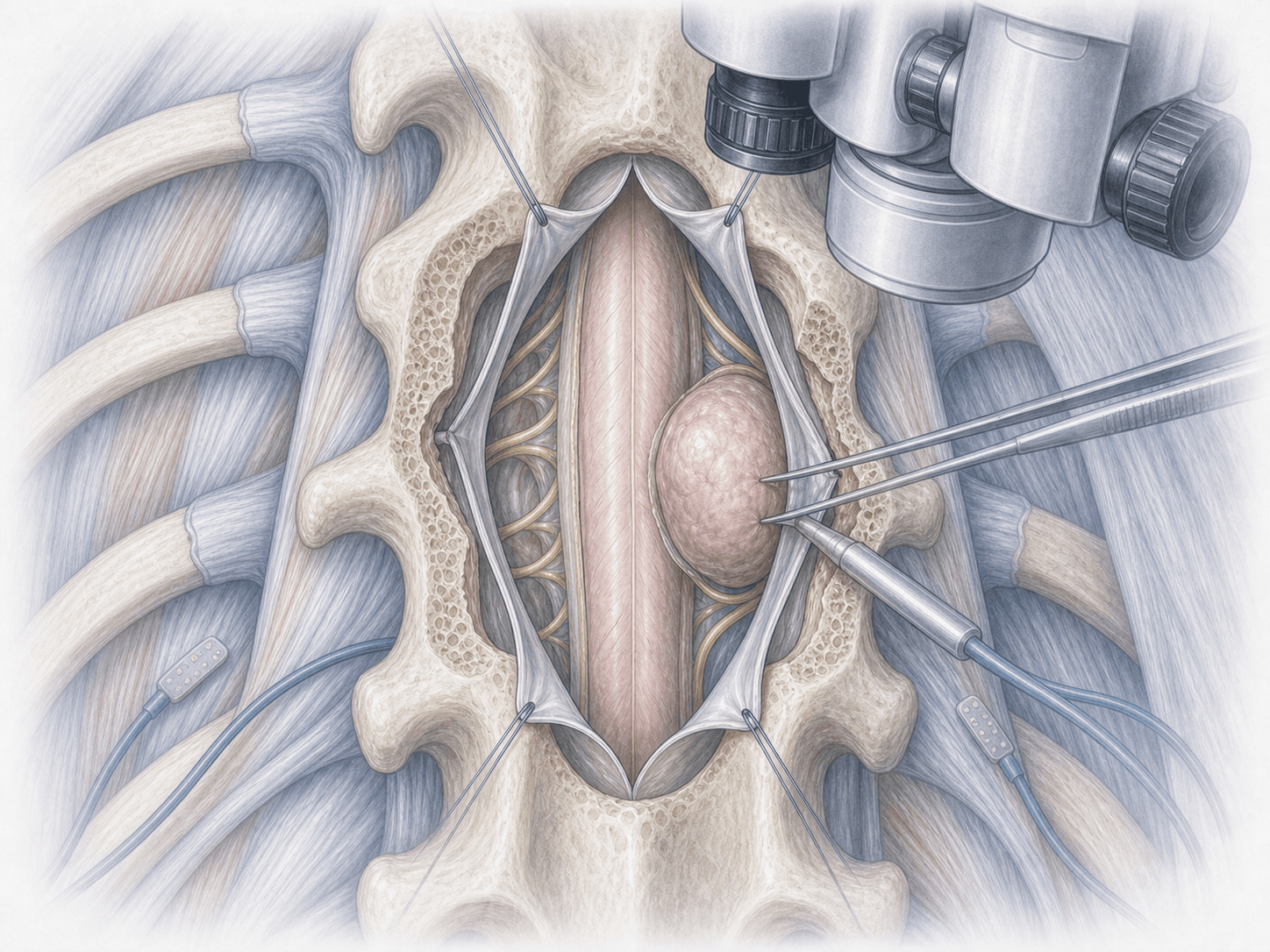
Thoracic microdiscectomy is a minimally invasive operation that we use to remove a dorsal disc herniation (between T1 and T12) under operating-microscope vision, through a small incision in the back. Unlike classical thoracic discectomy, here we work with continuous optical magnification, which lets us spare the neighbouring structures as much as possible: the spinal cord, the nerve roots and the facet joint.
The technical principle is clear: if we can decompress the cord without fully removing the facet, in most cases we do not need to add an instrumented fusion. That translates into a smaller scar, less postoperative pain and a faster recovery.
It is particularly useful for soft lateral or paramedian herniations. In markedly calcified, central herniations a different approach may be required (anterior transthoracic or lateral retropleural), and we discuss that with you during the consultation. To review your specific case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients we assess for a thoracic microdiscectomy usually report:
When is this procedure indicated?
How do we perform the procedure step by step?
1.Preoperative preparation
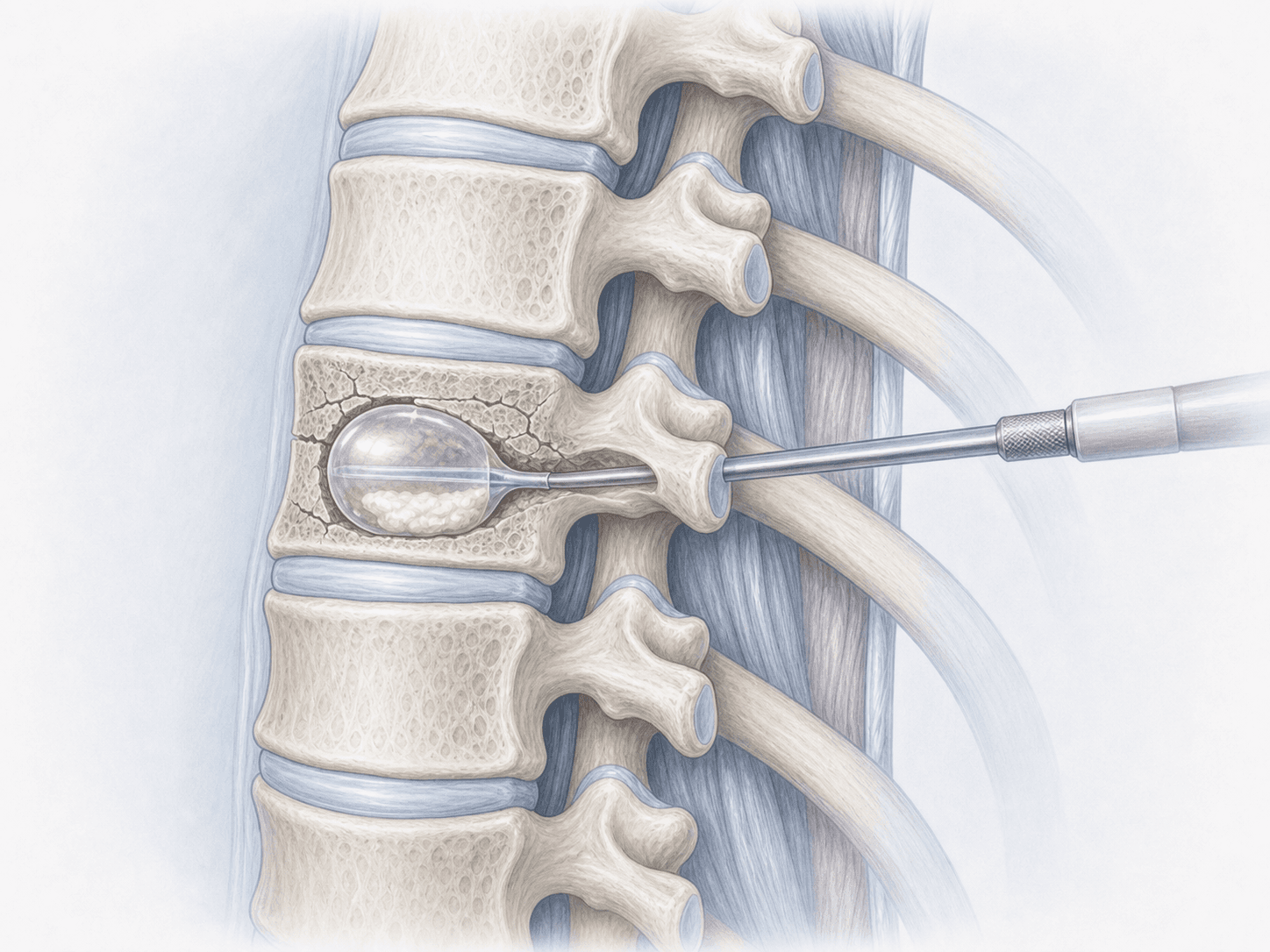
We review the MRI and, when needed, a CT scan to assess how calcified the herniation is and the anatomy of the pedicle. We confirm the exact level to be treated using intraoperative imaging. We explain the procedure in detail, hand over the informed consent and provide instructions on fasting and medication adjustments.
2.During the procedure
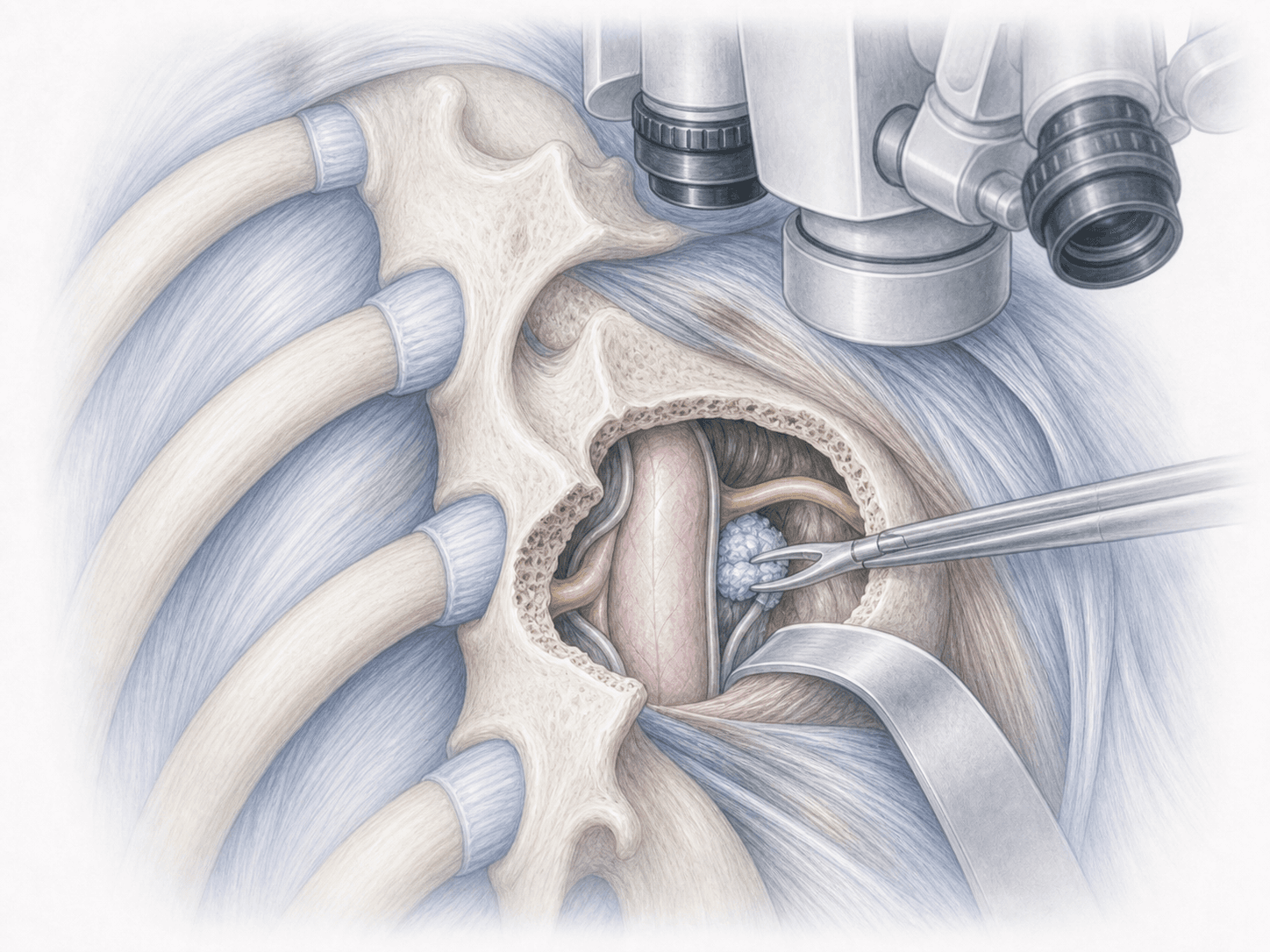
Under general anaesthesia and with intraoperative neuromonitoring, we position you in the prone decubitus. After locating the correct level with fluoroscopy, we make a small midline or paramedian incision.
We reach the disc through a posterolateral approach: in most cases a facet-sparing (pedicle-sparing) transfacet or a transpedicular route, which lets us see the cord from a lateral angle without manipulating it. Using the operating microscope, we remove the herniated portion of the disc and decompress the affected cord and nerve root. If the facet joint remains intact, we do not add any fusion.
3.Immediate postoperative period
After surgery you spend a short time in the recovery unit and then return to the ward. We start mobilisation the same day or within a few hours, monitor pain control and check your neurological status. Hospital stay is usually 2–3 nights depending on progress.
Recovery after a thoracic microdiscectomy
Recovery is gradual. Walking and light activity at home are usually possible from day one. Returning to office work typically occurs between 3 and 6 weeks, depending on wound healing and pain. Jobs involving physical effort require additional time.
Because in most cases there is no fusion, you do not need to wait for bone healing. We do ask you to avoid heavy lifting and impact sports during the first weeks, and to introduce physiotherapy progressively. Fever, markedly worsening pain, wound discharge or new neurological symptoms warrant prompt contact with us.
Risks and possible complications
Any surgical procedure carries general risks such as infection, bleeding, anaesthesia-related issues or venous thrombosis.
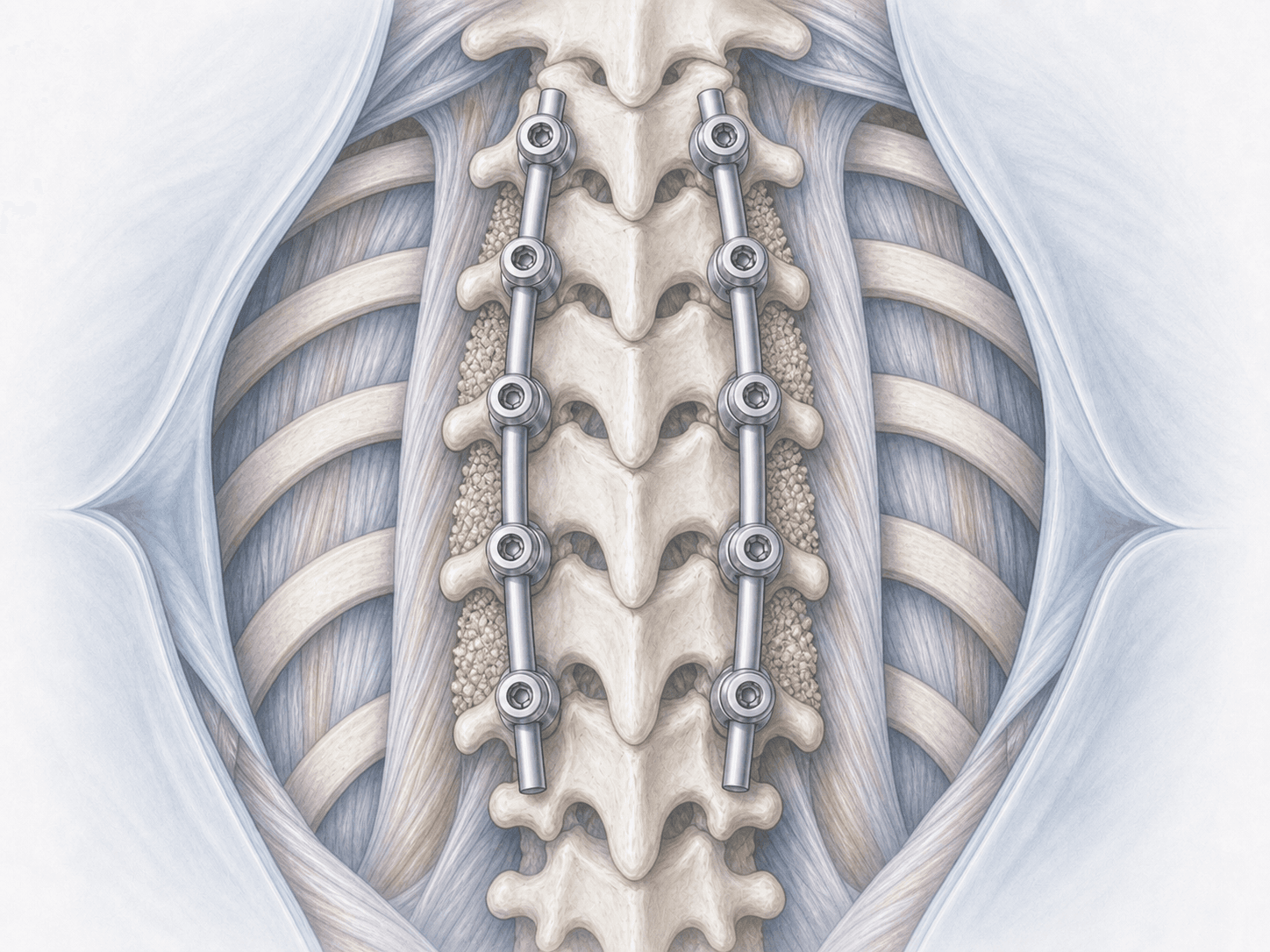
Specific risks of thoracic microdiscectomy include spinal cord or nerve root injury, cerebrospinal fluid leak, residual or recurrent herniation, persistent band-like neuropathic pain and, in a small minority of cases, postoperative instability that may require subsequent fusion. In markedly calcified, central herniations, if posterolateral exposure proves insufficient, conversion to a wider approach or a second intervention may be needed.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala