TLIF — Transforaminal lumbar interbody fusion
TLIF (transforaminal lumbar interbody fusion) is a surgical technique that combines nerve decompression and stabilisation of the lumbar segment. We approach the spine from the back, partially remove the facet joint and reach the disc through the foramen, which allows us to work from one side without retracting the dural sac across the midline. Many patients come to this option after months of low back pain and sciatica that do not improve, or with a slowly progressing spondylolisthesis. Others come after a recurrent disc herniation at the same level. This guide explains, realistically, what the surgery involves, when it is indicated and what recovery looks like, so you can make a calm, informed decision.
What is TLIF (transforaminal lumbar interbody fusion)?
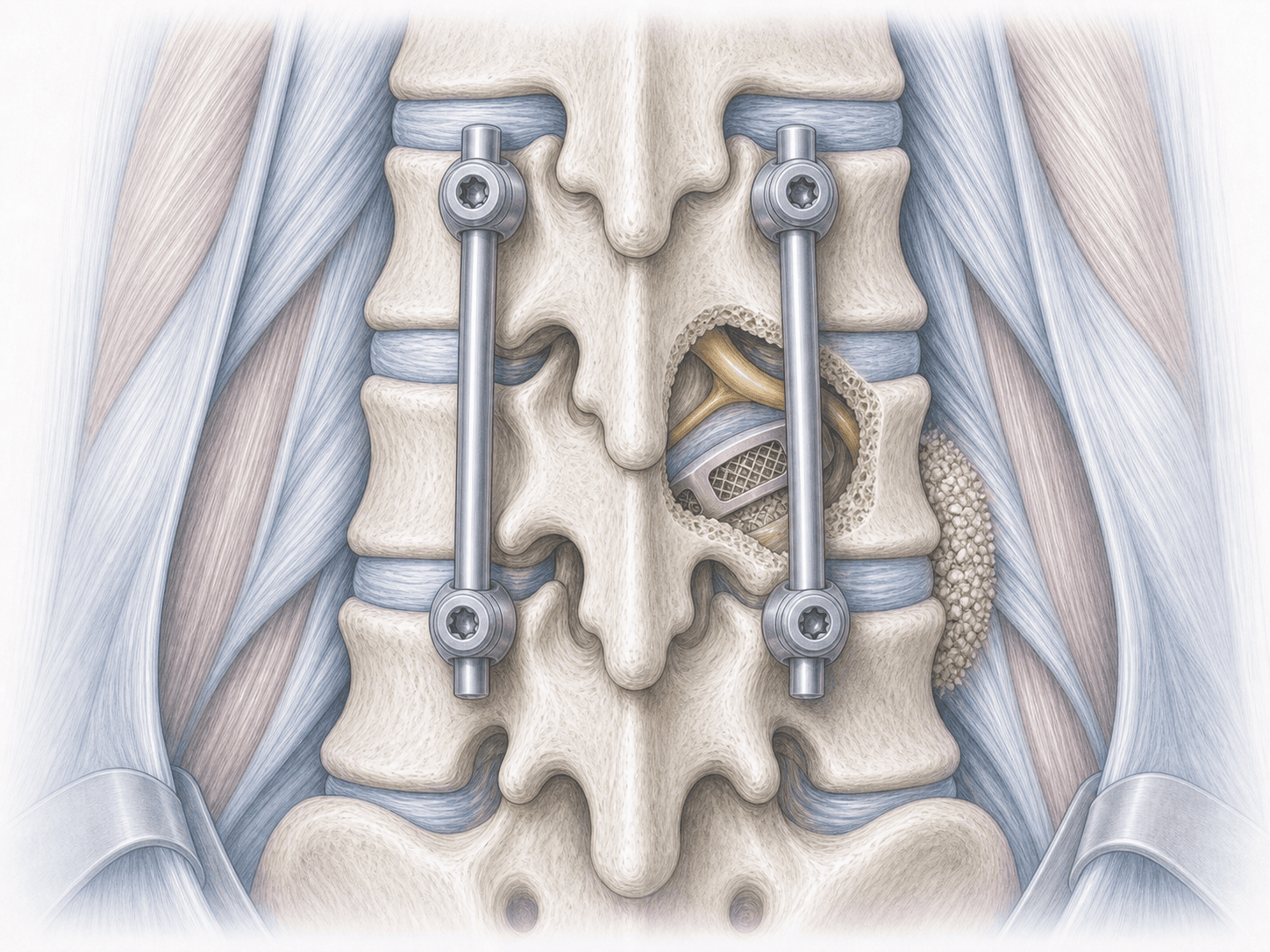
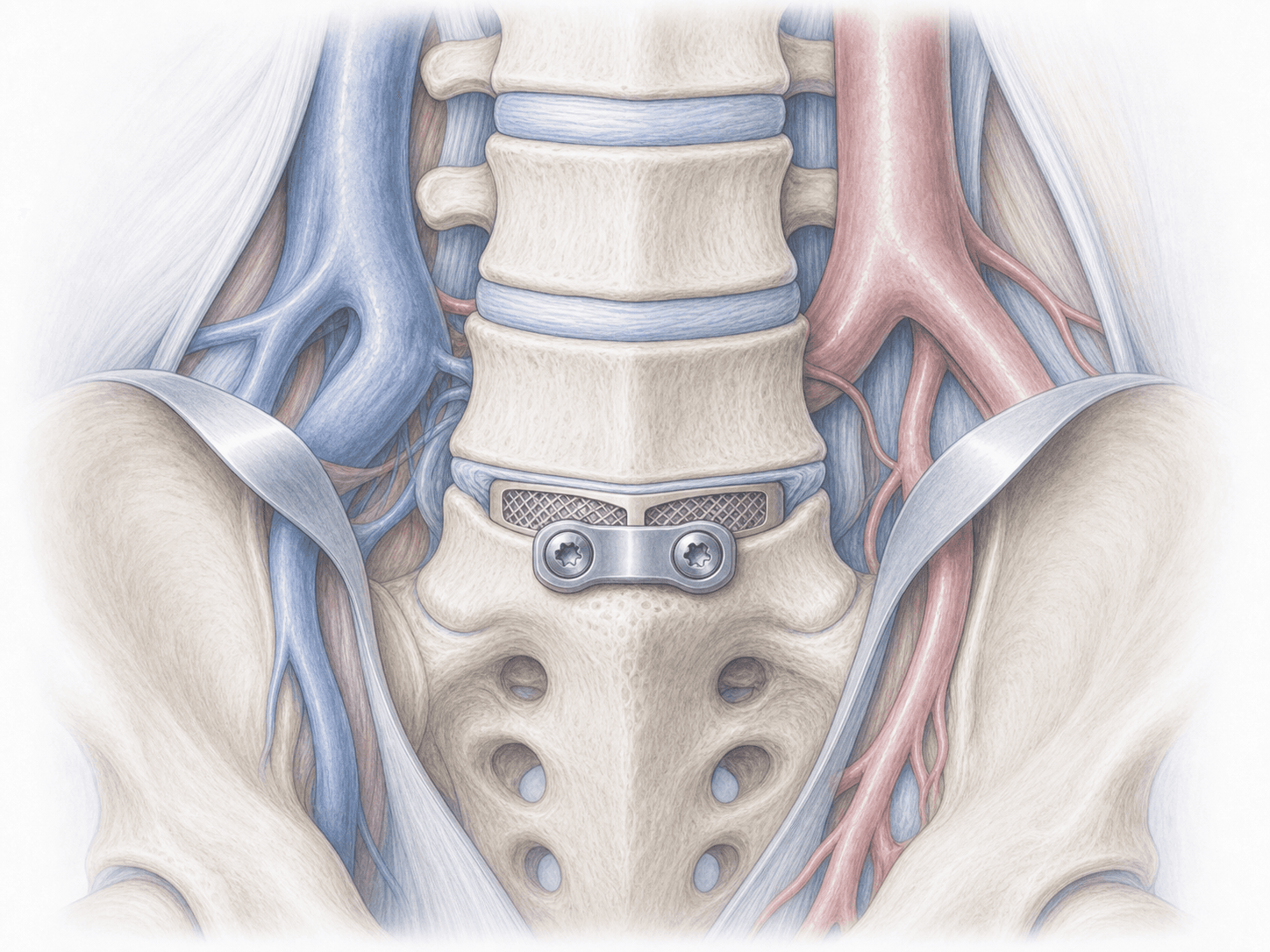
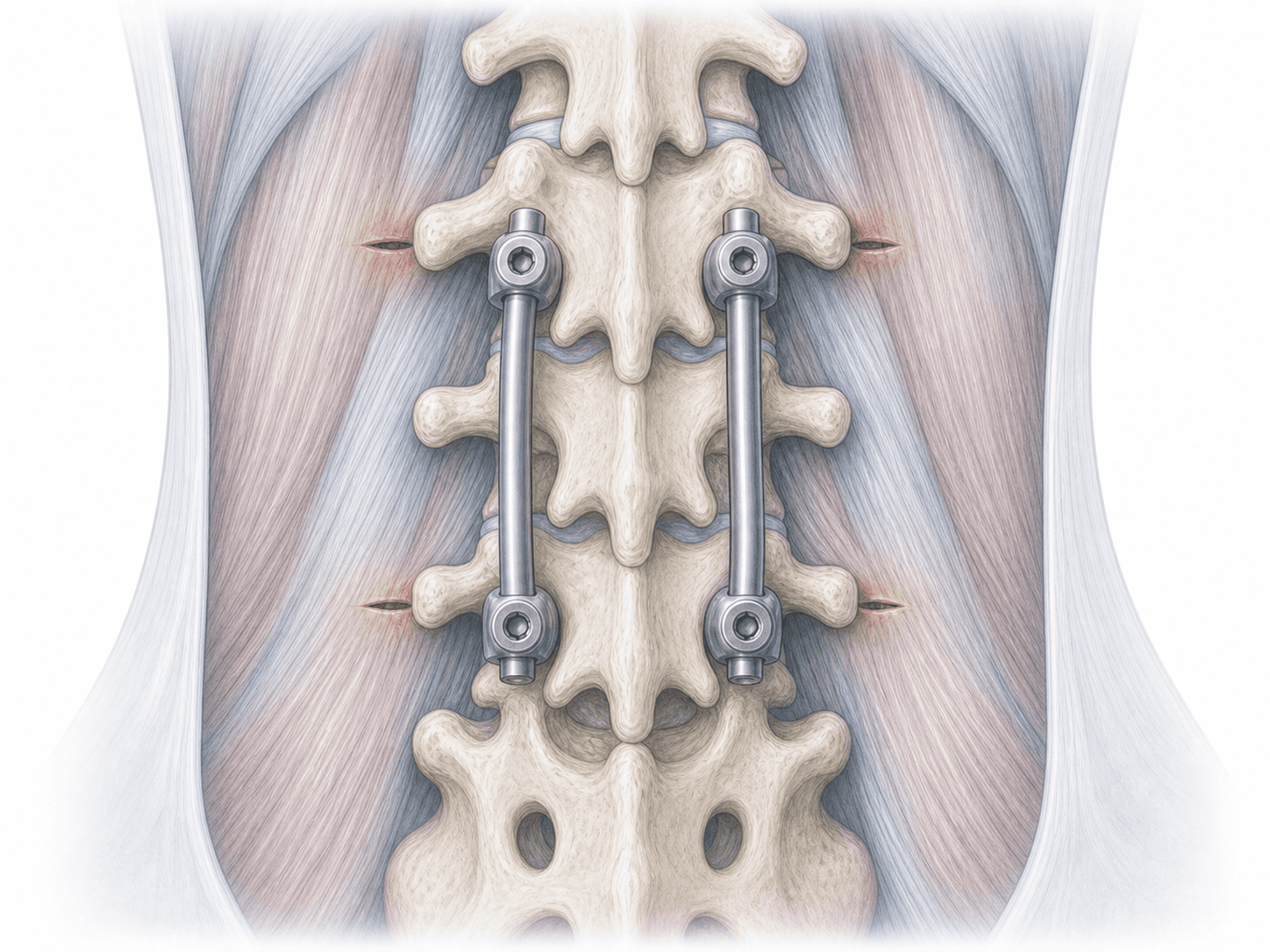
TLIF is a lumbar fusion technique performed through a posterolateral approach. We work from the back, partially remove the facet joint on the affected side and enter the disc through the foramen. Once inside, we clean the disc, decompress the nerve root, place a bone graft and an interbody cage, and stabilise the segment with pedicle screws connected by two rods.
Unlike PLIF, which enters through the midline and requires retraction of the dural sac on both sides, TLIF allows lateral access to the disc with less neural manipulation. Compared with ALIF (anterior approach) or XLIF (lateral approach), TLIF has the advantage of decompressing and stabilising in the same step, without requiring a second approach. To discuss your specific case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from TLIF typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
Before surgery we review the MRI and, if needed, dynamic X-rays or a CT scan to assess instability and bone quality. We carry out a full clinical assessment, review your current medication (especially anticoagulants and antiplatelet drugs), explain the procedure in detail and answer your questions. You will also receive fasting instructions and specific guidance for the day of the operation.
2.During the procedure
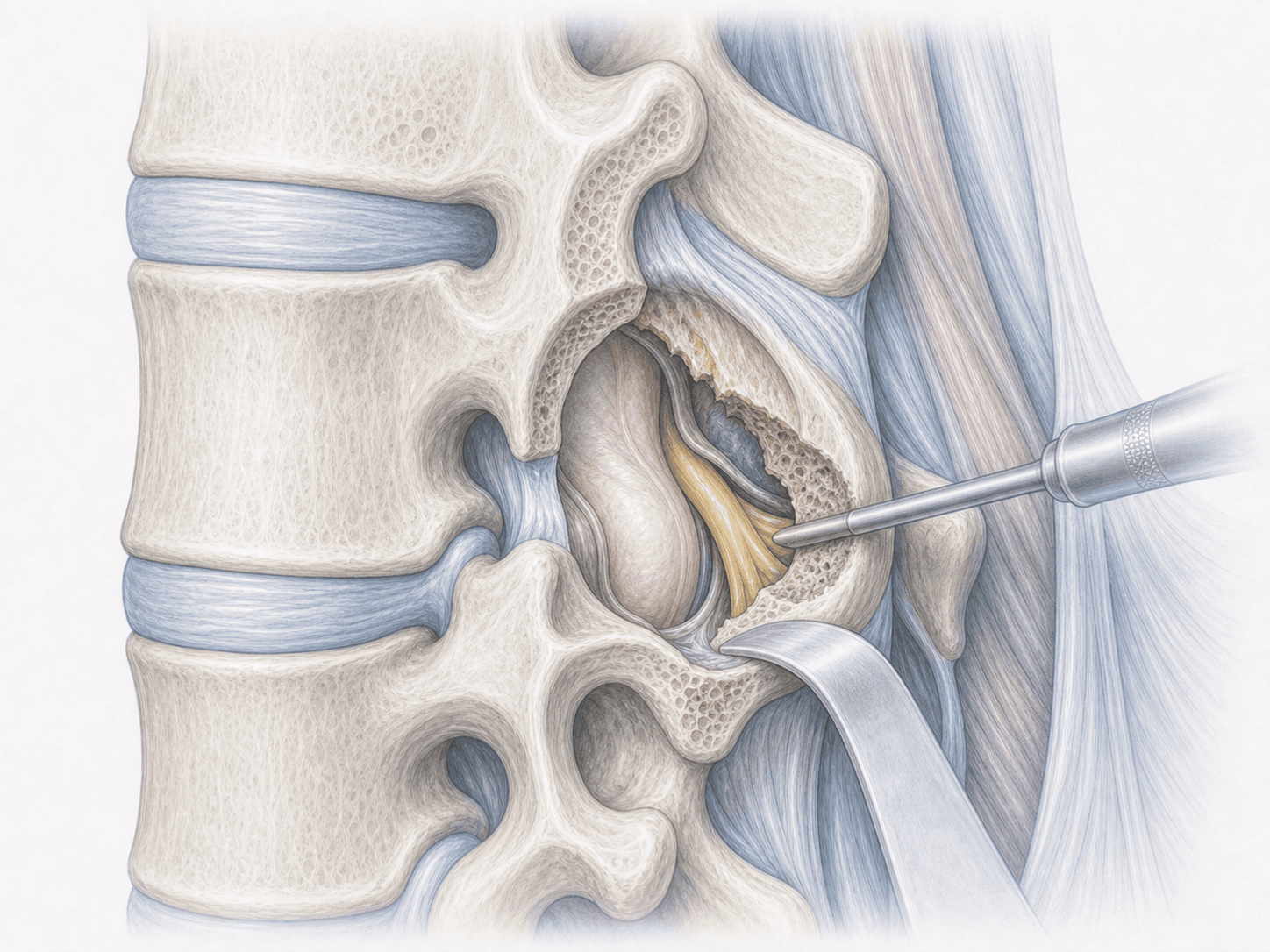
TLIF is performed under general anaesthesia with the patient in the prone position. We make a posterior approach and, under fluoroscopic guidance, place the pedicle screws in the vertebrae to be fused. We then partially remove the facet joint on the most symptomatic side to enter the disc through the foramen. The disc is cleaned, the nerve root decompressed and, once the space is freed, a bone graft and an interbody cage are inserted to restore disc height. Finally, the screws are connected by two rods to stabilise the segment and promote fusion.
3.Immediate postoperative period
After surgery you will spend a short time in recovery before returning to your room. We manage pain, check your neurological status and, as soon as possible, help you stand up and take your first steps, usually the day after surgery. Hospital stay is typically 3-5 days depending on clinical progress, and before discharge we will go through wound care and your rehabilitation plan with you.
Recovery after TLIF
Recovery after TLIF is gradual and best approached in stages. Walking daily, in short but frequent sessions, is the best early rehabilitation. Sedentary activities and driving are usually resumed between 4 and 6 weeks; physical jobs require longer, typically 2-3 months.
Bony fusion consolidates over several months, so avoiding heavy loads, sudden twisting and impact sports early on is essential. Physiotherapy is introduced gradually when we advise. Fever, severe pain that does not settle, wound discharge or new neurological symptoms warrant prompt medical review.
Risks and possible complications
Any surgery carries general risks such as infection, bleeding, deep vein thrombosis or anaesthesia-related complications.
Specific risks of TLIF include nerve root injury or a dural tear with cerebrospinal fluid leak, malposition of the pedicle screws, migration or subsidence of the interbody cage, non-union of the fusion (pseudarthrosis) and accelerated degeneration of adjacent levels in the medium to long term. These risks are assessed individually for each patient and explained in detail before signing the consent form.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala