XLIF / LLIF / OLIF — Lateral and oblique interbody fusions
Lateral interbody fusions (XLIF or LLIF, transpsoas with lumbar plexus neuromonitoring) and oblique fusions (OLIF, retroperitoneal pre-psoas) are minimally invasive techniques that place a wide cage between the vertebral bodies to restore disc height, lordosis and indirectly decompress the nerves. They are especially helpful at L1–L4 levels with degenerative disc disease, adult degenerative scoliosis, spondylolisthesis or foraminal stenosis, where a large cage stabilises the segment without disturbing the paraspinal muscles. This guide walks you through when the procedure is indicated, how recovery looks and which specific risks we monitor closely, particularly those involving the lumbar plexus.
What are XLIF, LLIF and OLIF?
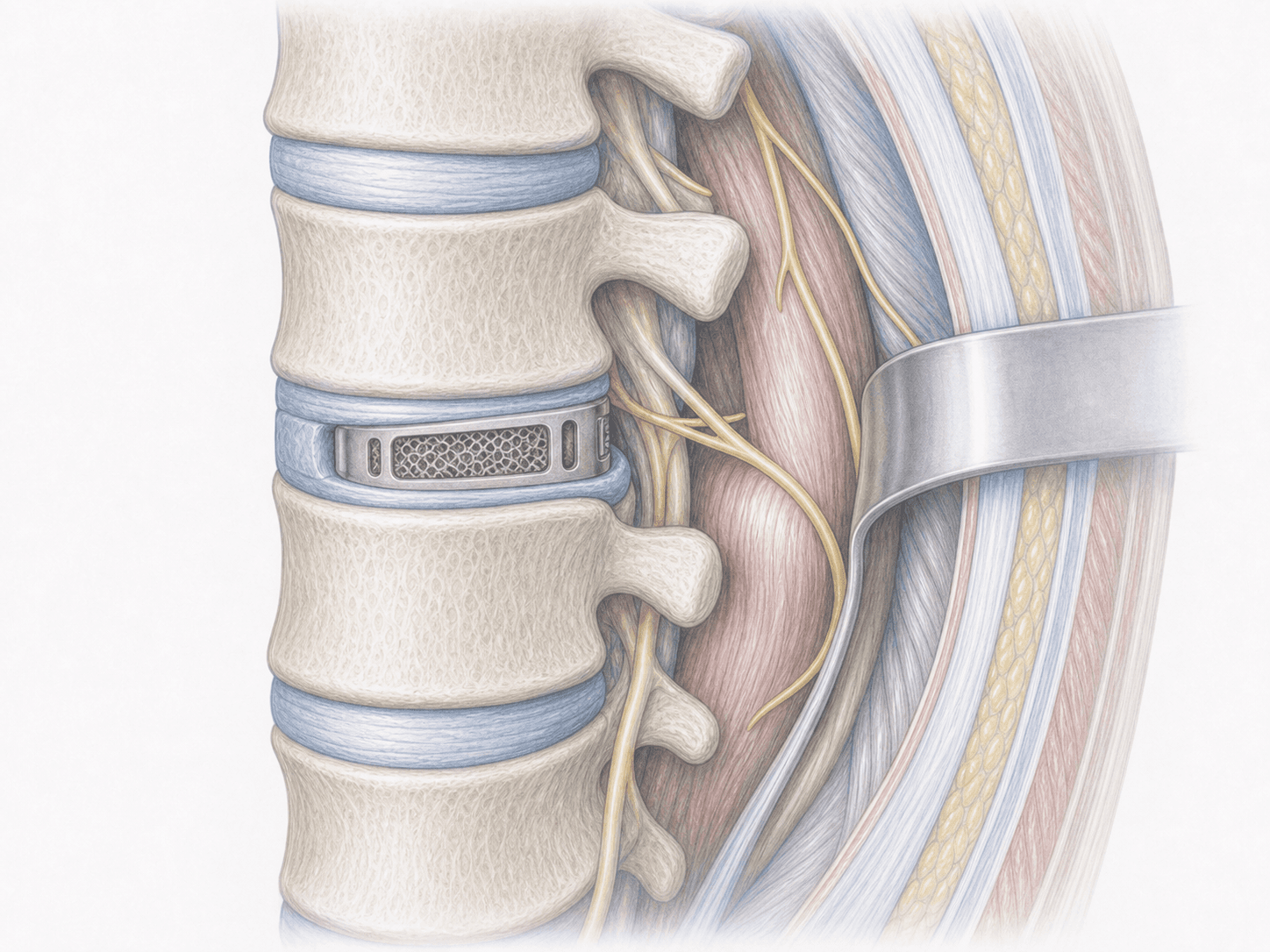
XLIF (eXtreme Lateral Interbody Fusion) and LLIF (Lateral Lumbar Interbody Fusion) describe the same family of technique: we reach the lumbar spine through a lateral abdominal corridor, gently passing through the psoas muscle with a dilator under continuous lumbar plexus neuromonitoring to locate and protect the nerve roots. OLIF (Oblique Lateral Interbody Fusion) uses a slightly more anterior, retroperitoneal route in front of the psoas, without going through it.
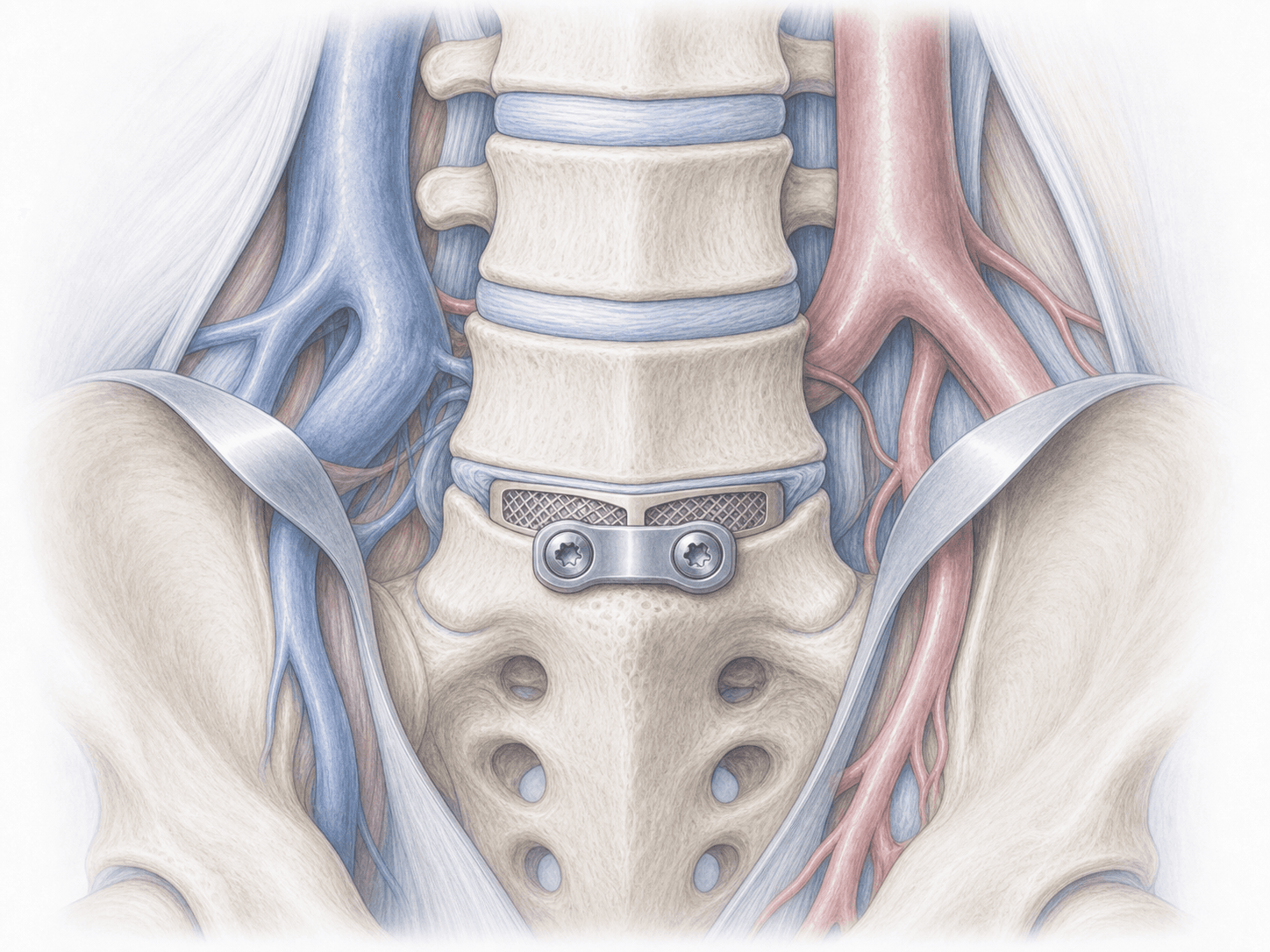
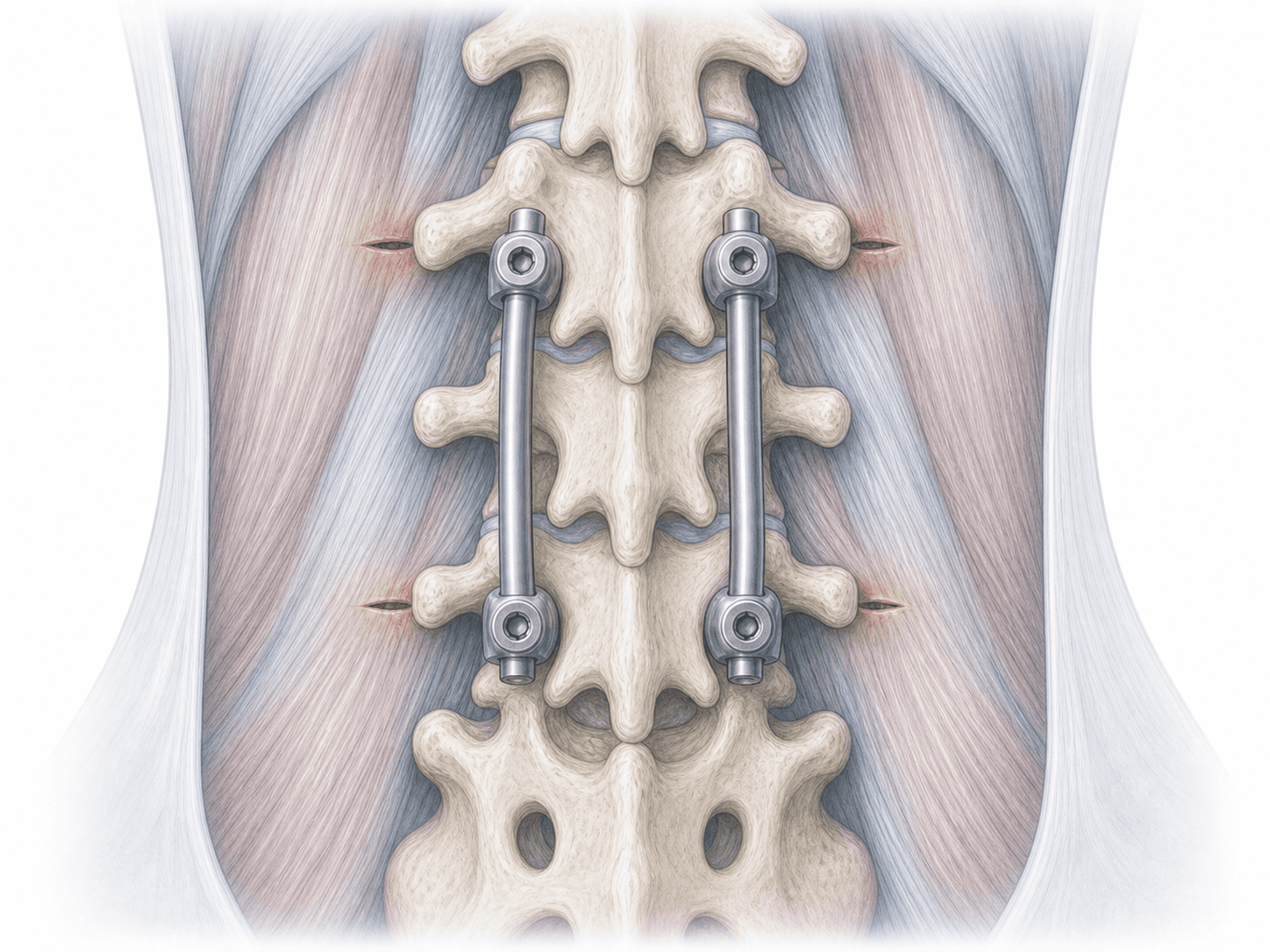
In all three approaches we remove the damaged disc and place a wide interbody cage that rests on the strong vertebral endplates and restores disc height and lordosis. This large cage decompresses the nerves indirectly and, in many cases, avoids the need for posterior screws or allows them to be added percutaneously in a less invasive way. Unlike ALIF, the lateral or oblique route is usually reserved for L1–L4: at L5–S1, the iliac crest and vascular anatomy make an anterior approach more suitable. To check whether your case fits, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from a lateral or oblique fusion typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
We review the MRI, standing X-rays and, in scoliosis cases, full-length spine radiographs. We assess the height of the iliac crest and the position of the lumbar plexus to choose between XLIF/LLIF or OLIF at each level. We give fasting instructions, adjust medication (anticoagulants, anti-inflammatories) and discuss the anaesthetic plan and the neuromonitoring set-up with you.
2.During the procedure
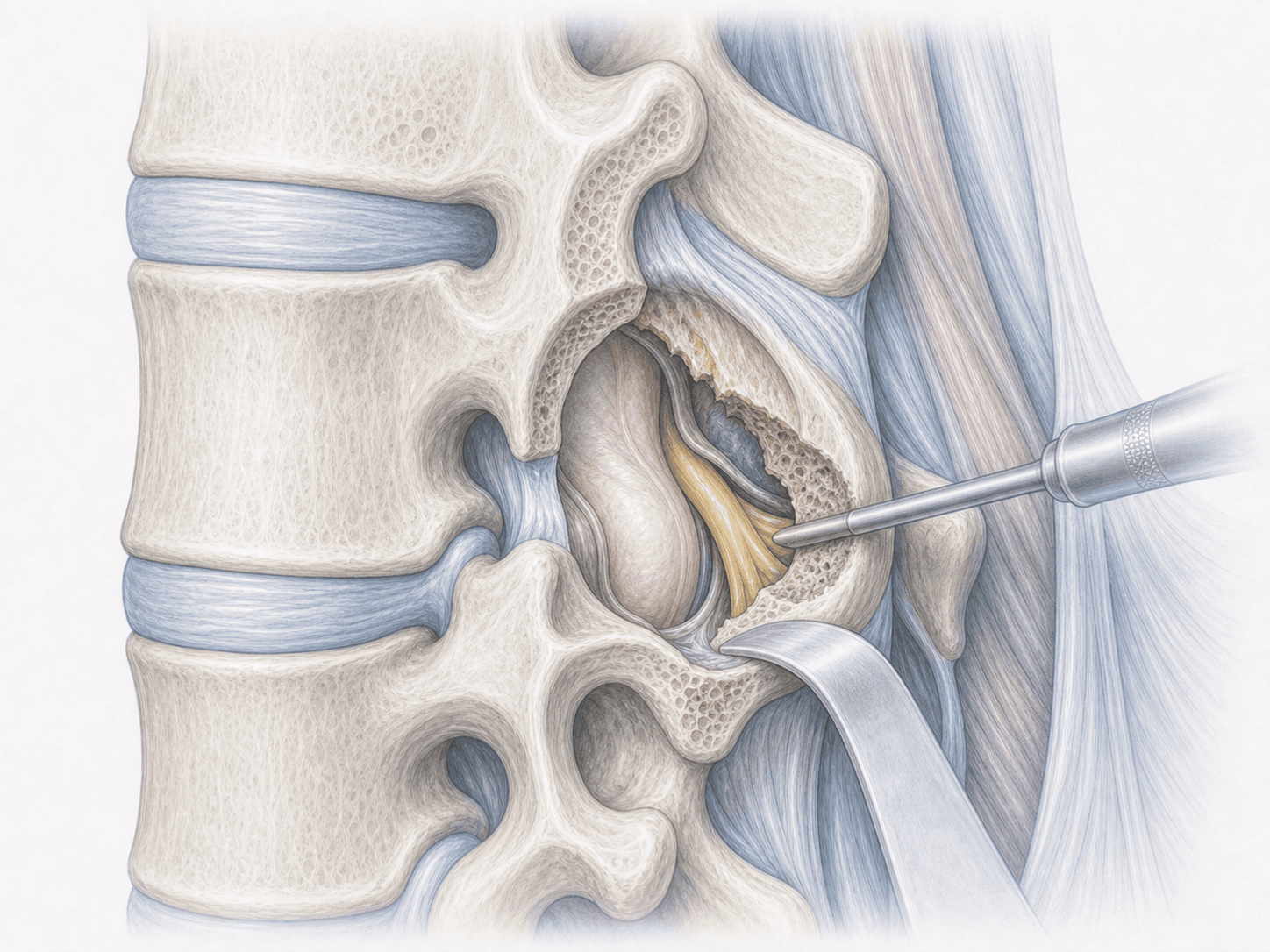
Under general anaesthesia we position you in the lateral decubitus, firmly secured to the table. We make a small flank incision, enter the retroperitoneal space and, in XLIF/LLIF, traverse the psoas with a dilator and continuous lumbar plexus neuromonitoring. In OLIF we advance in front of the psoas. Once at the disc level, we remove the damaged nucleus, prepare the vertebral endplates and place a wide interbody cage filled with bone graft. If the case requires it, we complement the fusion with percutaneous pedicle screws during the same procedure or in a second stage.
3.Immediate postoperative period
You spend a few hours in recovery and then return to your room. We control the pain, check leg strength and sensation to detect any lumbar plexus involvement early, and usually encourage you to stand up the same day or the next. Hospital stay is usually 2–4 nights depending on complexity and the number of levels treated.
Recovery after XLIF, LLIF or OLIF
Recovery after a lateral or oblique fusion is usually faster than after extensive posterior approaches because we preserve the paraspinal muscles. In the first weeks it is common to feel flank discomfort and transient psoas weakness or a sense of heaviness in the hip on the approached side: this is expected and generally improves over 4–8 weeks with targeted rehabilitation.
Light daily activities resume in a few days. Office work usually restarts in 3–6 weeks; physical jobs take longer. Bony fusion takes several months, so we avoid major strain early on and reintroduce sport gradually. If you develop fever, pain or new leg weakness, contact us without delay.
Risks and possible complications
Any surgery carries general risks: infection, bleeding, venous thrombosis or anaesthesia-related issues. For XLIF/LLIF and OLIF specifically, the unique risks come from the lateral abdominal corridor.
The most relevant are: transient lumbar plexus involvement (weakness or numbness in the front of the thigh, temporary psoas or quadriceps weakness), flank discomfort, hip pain when walking during the first weeks, vascular injury (uncommon but serious, particularly in OLIF due to proximity to the great vessels), incisional hernia, visceral injury, cage subsidence or pseudarthrosis. Choosing XLIF/LLIF versus OLIF for each level and the systematic use of neuromonitoring help us keep these risks to a reasonable minimum.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala