Posterior lumbar interbody fusion (PLIF)
Posterior lumbar interbody fusion (PLIF) is a surgical option for mechanical low back pain, persistent sciatica or instability when the problem stems from a degenerated disc, a spondylolisthesis or a stenosis that no longer responds to conservative care. Through a midline incision in the back we reach the spinal canal, decompress the nerve roots, remove the diseased disc and place two interbody cages together with pedicle screws and rods. The goal is twofold: take the pressure off the nerves and restore stability to the segment. This guide walks you through what to expect before, during and after the procedure, in plain language, so you can make a calm and informed decision.
What is posterior lumbar interbody fusion (PLIF)?
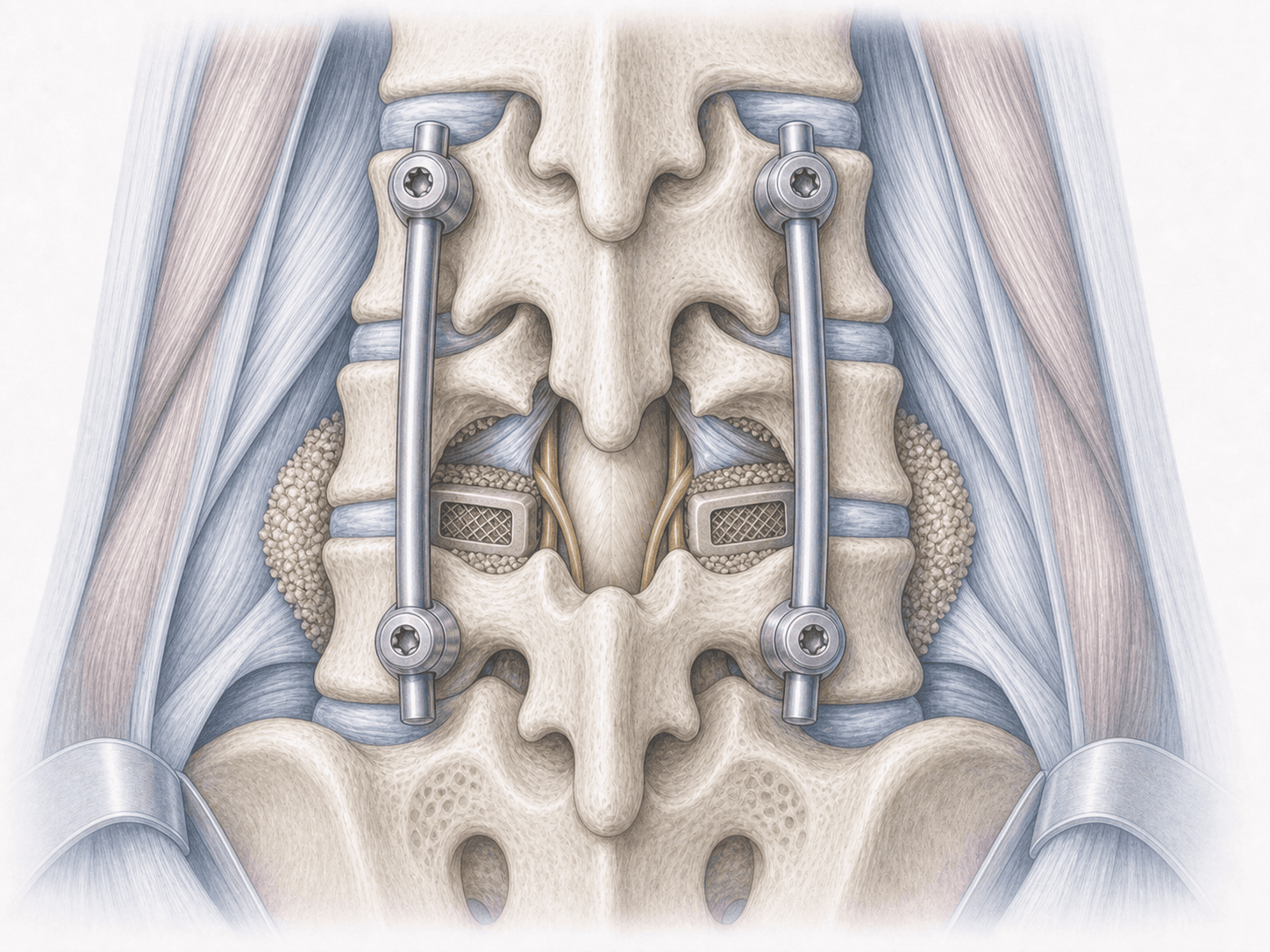
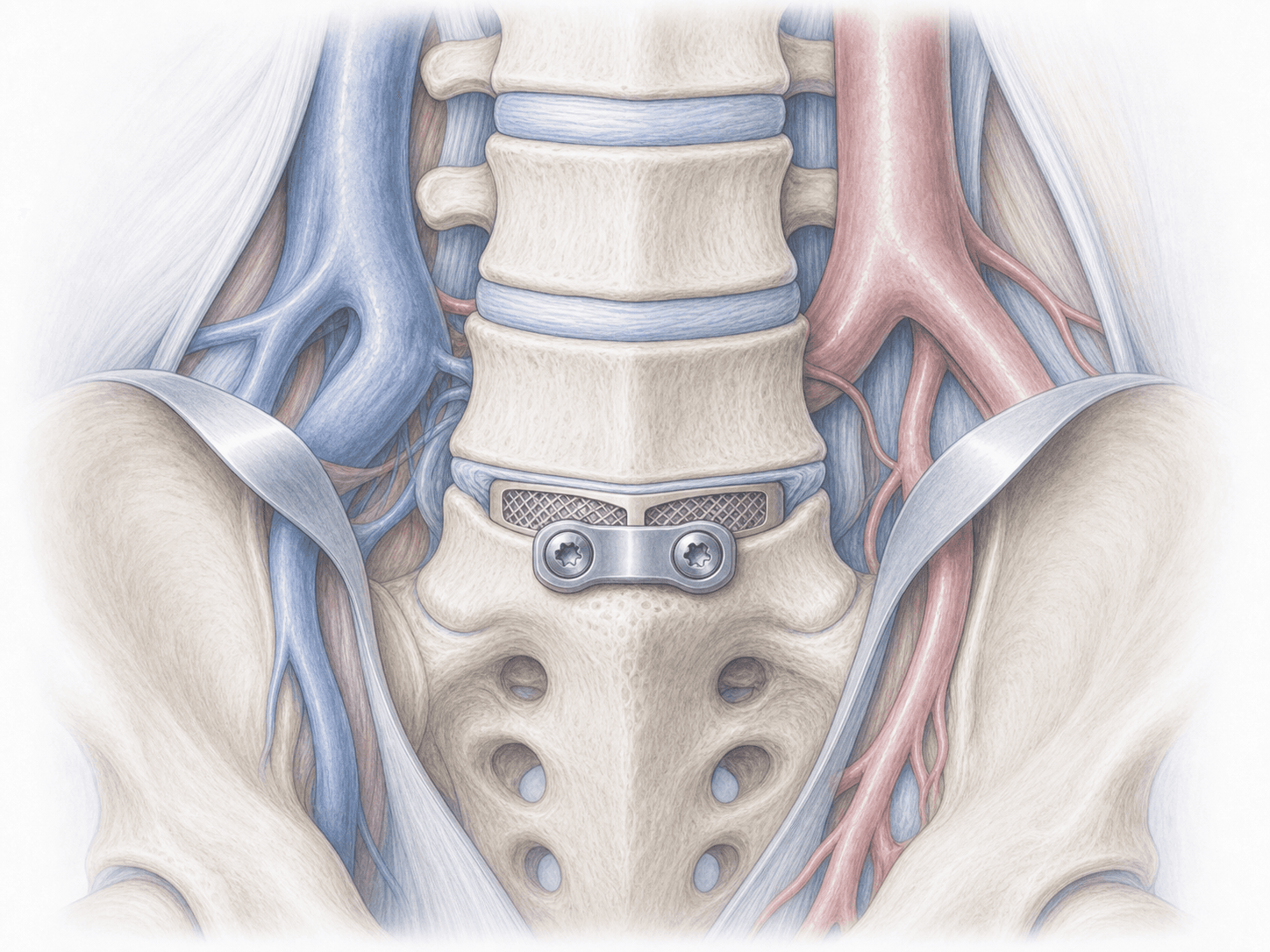
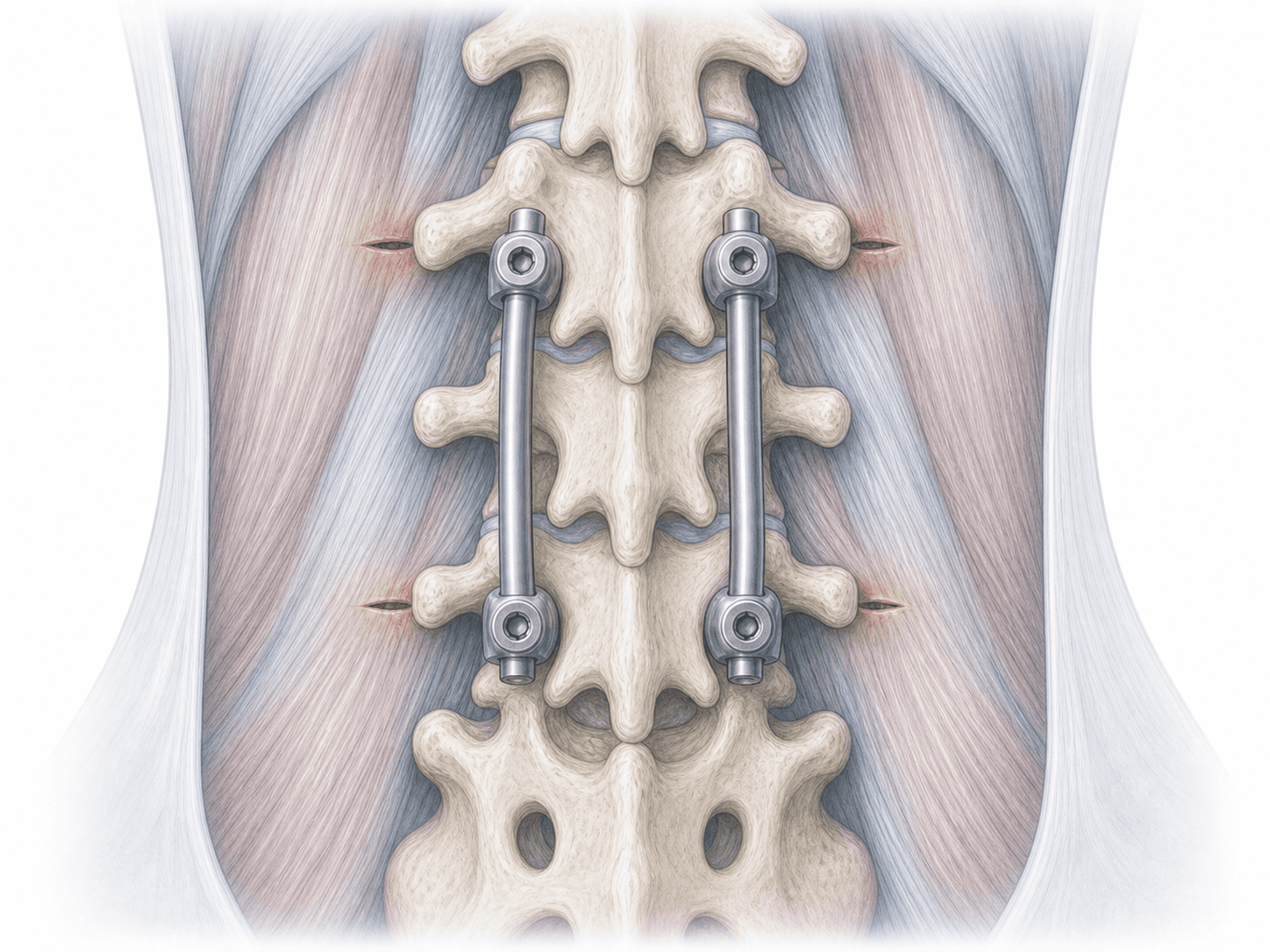
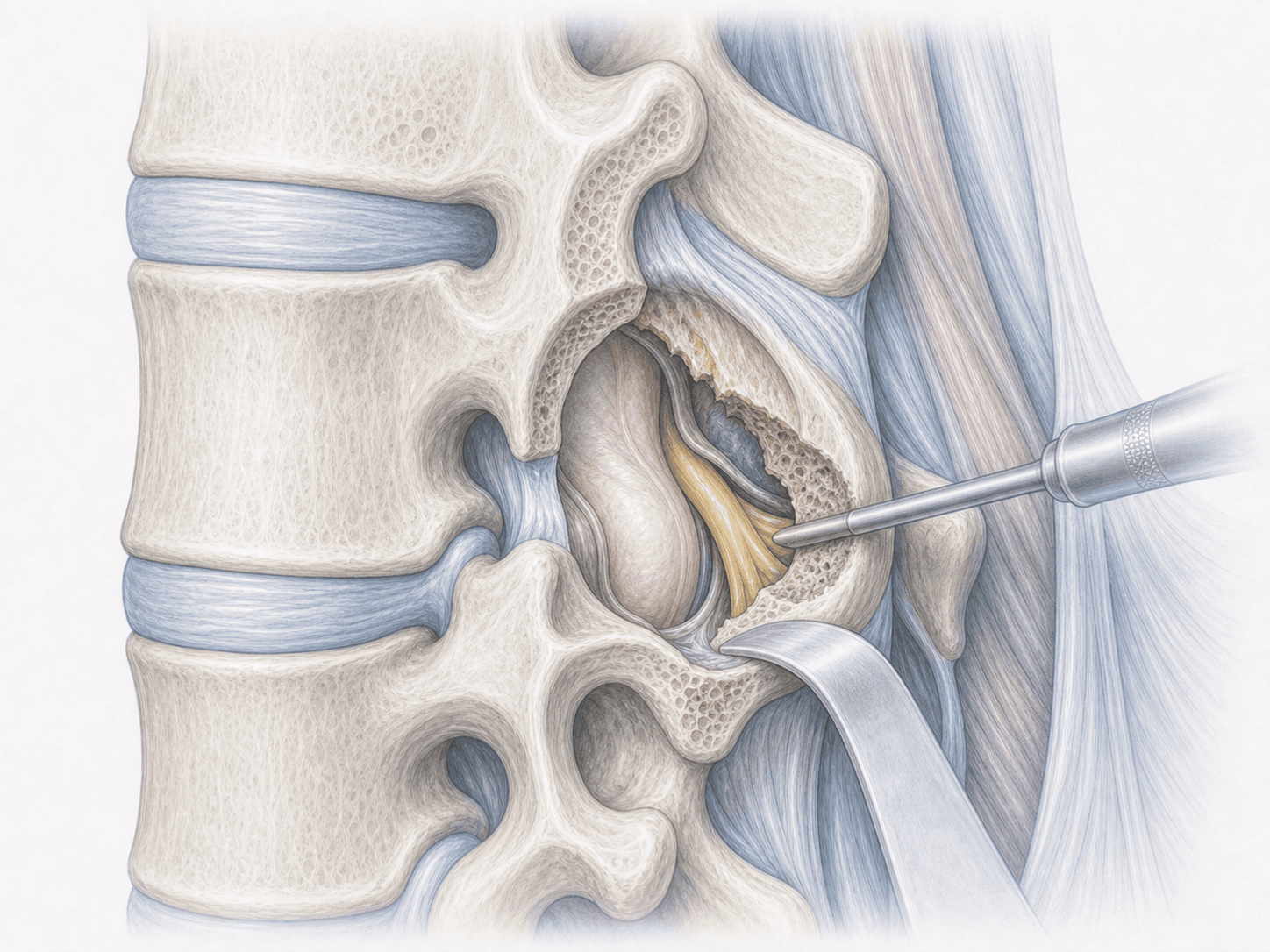
PLIF is a lumbar fusion technique in which we reach the spine through the back, along the midline. We perform a laminectomy and a partial facetectomy to access the disc, remove the damaged disc material and, after carefully retracting the dural sac and nerve roots, place two interbody cages (one on each side) within the disc space. We then fix the segment with pedicle screws and rods, which provides immediate stability and supports definitive bony fusion over the following months.
The key difference with transforaminal lumbar interbody fusion (TLIF) lies in dural retraction: PLIF approaches the disc from both sides of the midline, so the dural sac and the roots are handled a bit more, but it allows excellent central canal decompression and the placement of two symmetrical cages. The technique is particularly useful in significant central stenosis or when balanced correction on both sides of the disc is preferred.
If you think your case could fit, you can request an assessment with Dr. Ben Ghezala to review imaging, examination and realistic options.
Symptoms and warning signs
Patients who may benefit from PLIF usually describe a pattern similar to this:
When is this surgery indicated?
How is the procedure performed?
1.Preoperative preparation
Before surgery we review your MRI, dynamic X-rays (flexion-extension) and, if needed, CT to plan cage size and position as well as screw placement. We arrange preoperative blood tests, anaesthetic assessment and medication review, especially for anticoagulants and antiplatelets. We walk you through fasting instructions, what to bring to the hospital and what the first night after surgery will look like.
2.During the procedure
The procedure is performed under general anaesthesia, with you face down on the table and full radiological control. Through a midline incision in the back we access the segment, perform a laminectomy and a bilateral partial facetectomy, and decompress the canal and nerve roots. After careful retraction of the dural sac, we remove the diseased disc and place two interbody cages filled with bone graft, one on each side. We then fix the segment with pedicle screws and rods, check alignment and implant position and close the wound in layers. The procedure is performed under neuromonitoring to protect nerve function.
3.Immediate postoperative period
After surgery you spend some time in recovery and, once stable, return to your room. On the first day we usually get you sitting up and taking your first steps with help from the physiotherapist. Pain is managed with a combined regimen and we monitor neurological signs. The usual hospital stay is 3 to 5 days, depending on recovery, pain control and walking autonomy.
Recovery after PLIF
Recovery is gradual and benefits from a calm, staged plan. During the first 2-3 weeks the focus is short, repeated walks throughout the day, good sleep and avoiding prolonged postures or loads. Between weeks 4 and 8 most daily activities are resumed and supervised active rehabilitation begins.
Return to office work usually happens between weeks 4 and 6; physical jobs or those involving heavy lifting take 3-6 months. Bony fusion matures over 6-12 months, so we recommend caution with impact and loading throughout the first year. Rehabilitation, workplace ergonomics and clinical follow-up have a real impact on the final result.
Fever, pain that worsens rather than improves, wound drainage or new neurological symptoms require immediate medical assessment.
Risks and possible complications
All spine surgery carries general risks such as infection, bleeding, deep vein thrombosis or anaesthesia-related issues; in healthy patients these are uncommon but need to be known.
Specific PLIF risks include injury to a nerve root or the dural sac (with possible cerebrospinal fluid leak) related to the dural retraction this approach requires; malposition, migration or subsidence of the interbody cages; loosening or malposition of the pedicle screws; failure of the fusion to consolidate (pseudarthrosis); and accelerated degeneration of adjacent levels in the medium to long term. These risks are assessed case by case and are part of the decision between PLIF, TLIF or another alternative.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala