Thoracic vertebroplasty
Thoracic vertebroplasty is a minimally invasive percutaneous procedure in which we inject bone cement (PMMA) directly into the body of a fractured thoracic vertebra to stabilise it and reduce pain. It is designed for patients with osteoporotic or pathological vertebral fractures (caused by tumour or metastasis) who continue to experience severe, disabling pain after 2–3 weeks of conservative treatment with rest, analgesia and, often, a brace. This guide explains what the procedure involves, when it is indicated, what the day of surgery looks like and what to expect afterwards, so you can decide calmly and with clear information.
What is thoracic vertebroplasty?
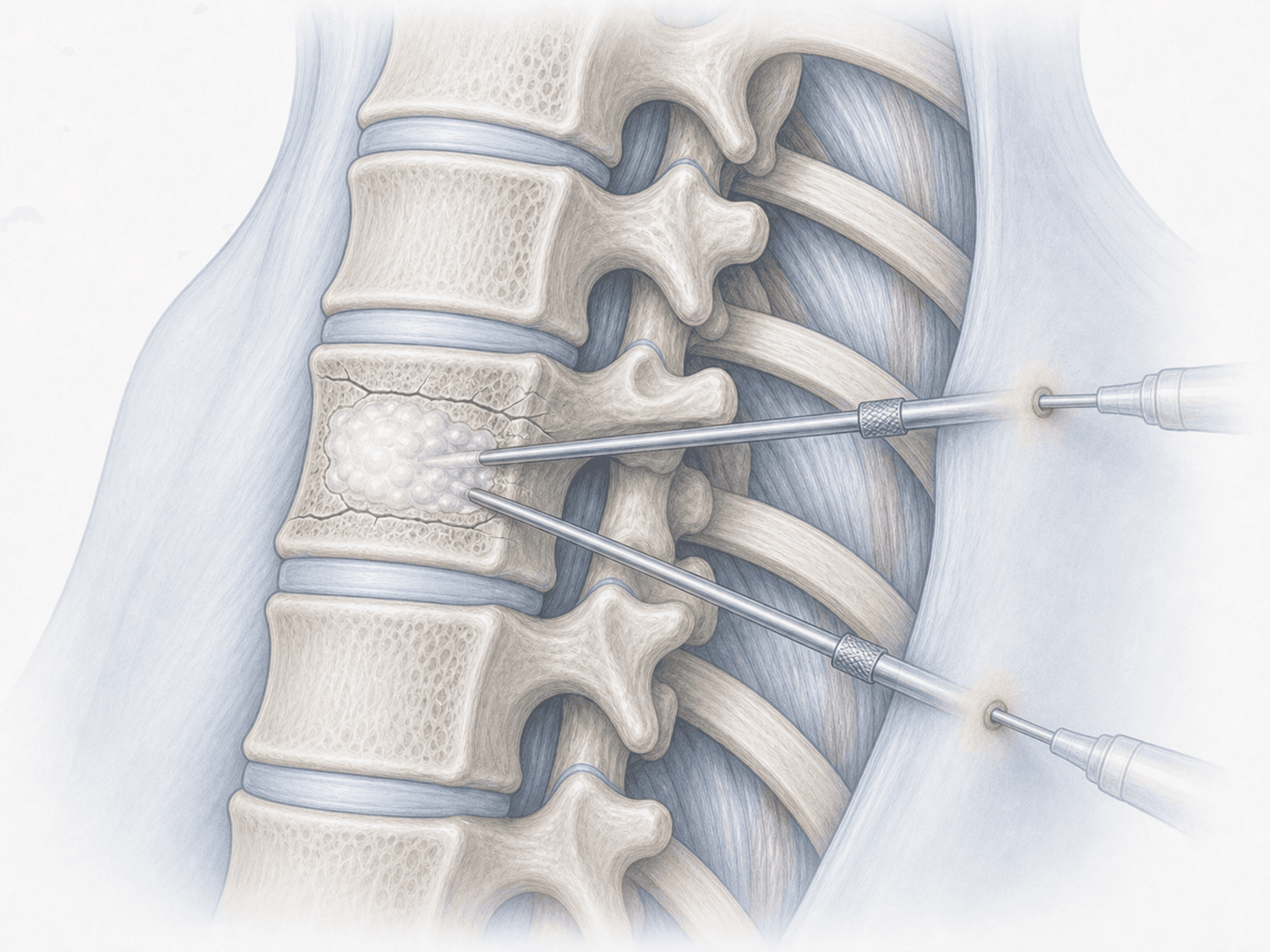
Thoracic vertebroplasty is a percutaneous technique in which, under image guidance, we introduce a needle or trocar through the pedicle of the fractured thoracic vertebra and inject bone cement (polymethylmethacrylate, or PMMA) directly into the vertebral body. The cement hardens in a few minutes, stabilises the microfractures and reduces pain.
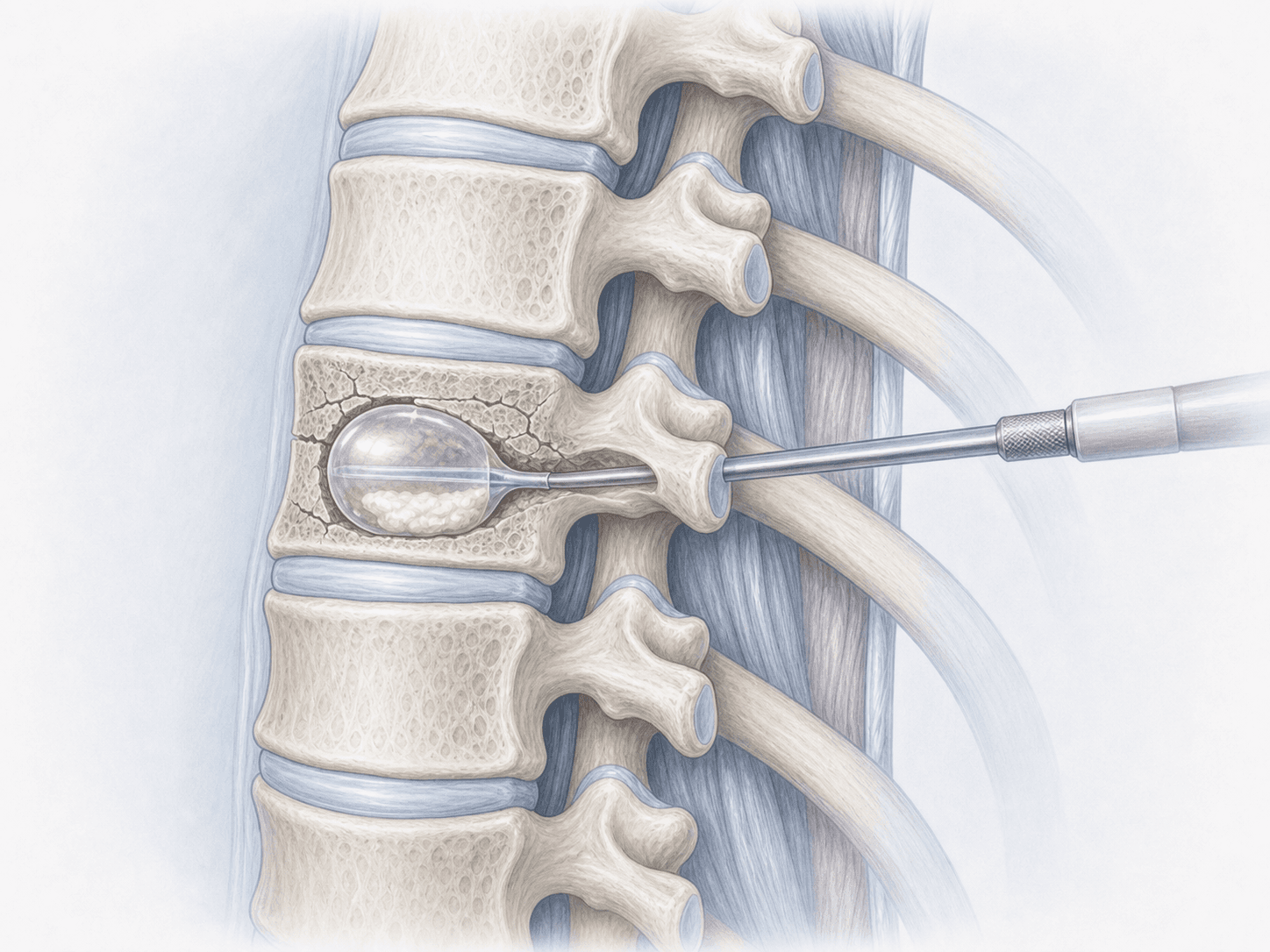
Unlike thoracic kyphoplasty, which uses a balloon to create a cavity and partially restore vertebral height before injecting cement, vertebroplasty injects the PMMA directly, without a balloon. For that reason we reserve vertebroplasty for stable fractures without significant height loss, where the main goal is pain control and stabilisation of the vertebra. If you are unsure which option is best for your case, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from thoracic vertebroplasty typically describe:
When is thoracic vertebroplasty indicated?
How is the procedure performed?
1.Preoperative preparation
Before the vertebroplasty we review the MRI and, if needed, the CT scan to confirm that the fracture is recent (bone marrow oedema) and suitable for this technique. We check coagulation, adjust medication (especially anticoagulants) and provide fasting instructions. We answer your questions and plan together either a same-day discharge or a 24-hour stay depending on the case.
2.During the procedure
The patient lies face down. Thoracic vertebroplasty is usually performed under local anaesthesia and sedation, although in some cases we choose general anaesthesia. Under continuous fluoroscopic guidance we introduce one or two fine trocars through the pedicle (or through an extrapedicular route at upper levels such as T4–T8) into the vertebral body. Once correctly positioned, we inject the PMMA cement with strict image control to avoid leakage. The procedure takes 30 to 60 minutes per level and requires no surgical incision — only two small skin punctures.
3.Immediate postoperative period
After the procedure patients remain lying down for 1 to 2 hours to let the cement fully harden. They then sit up and start walking with staff support. Most patients notice a clear improvement in pain within the first hours. Discharge is typically the same day or within 24 hours, depending on the patient's baseline status and pain control.
Recovery after thoracic vertebroplasty
Recovery is fast compared with open surgery. Most patients walk again on the same day and return to everyday activities within a few days.
During the first 2–4 weeks we ask patients to avoid heavy effort, lifting significant weight or sharp spinal flexion. In patients with osteoporosis, the underlying medical treatment (calcium, vitamin D, antiresorptive or anabolic drugs) is key to reducing the risk of new fractures at other levels. In oncological patients we coordinate the plan with their oncology and radiotherapy team.
Any recurrence of pain, fever, leg weakness or new neurological changes should be reviewed immediately.
Risks and possible complications
Any procedure carries general risks such as infection, bleeding, reaction to anaesthesia or cardiopulmonary complications.
The most characteristic risk of vertebroplasty is cement leakage outside the vertebral body. Most leakages are small and asymptomatic, but in rare cases they may affect veins, the disc, the spinal canal or the foramen, causing pain, nerve root irritation or, exceptionally, pulmonary cement embolism. Other possible risks include rib or pedicle fracture, neurological injury and the appearance of new vertebral fractures at adjacent levels due to the underlying bone fragility. We assess each case individually and discuss the risks in detail before deciding.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala