Percutaneous thoracic instrumentation
Percutaneous thoracic instrumentation is a minimally invasive (MIS) fixation technique that stabilises one or several levels of the thoracic spine using pedicle screws placed through small skin incisions, without detaching the paraspinal muscles. It is an alternative to the open approach for selected fractures, vertebral metastases or infections, preserving soft tissues and supporting a faster recovery. This guide explains when the procedure is indicated, how it is performed with intraoperative navigation and what to expect during and after surgery.
What is percutaneous thoracic instrumentation?
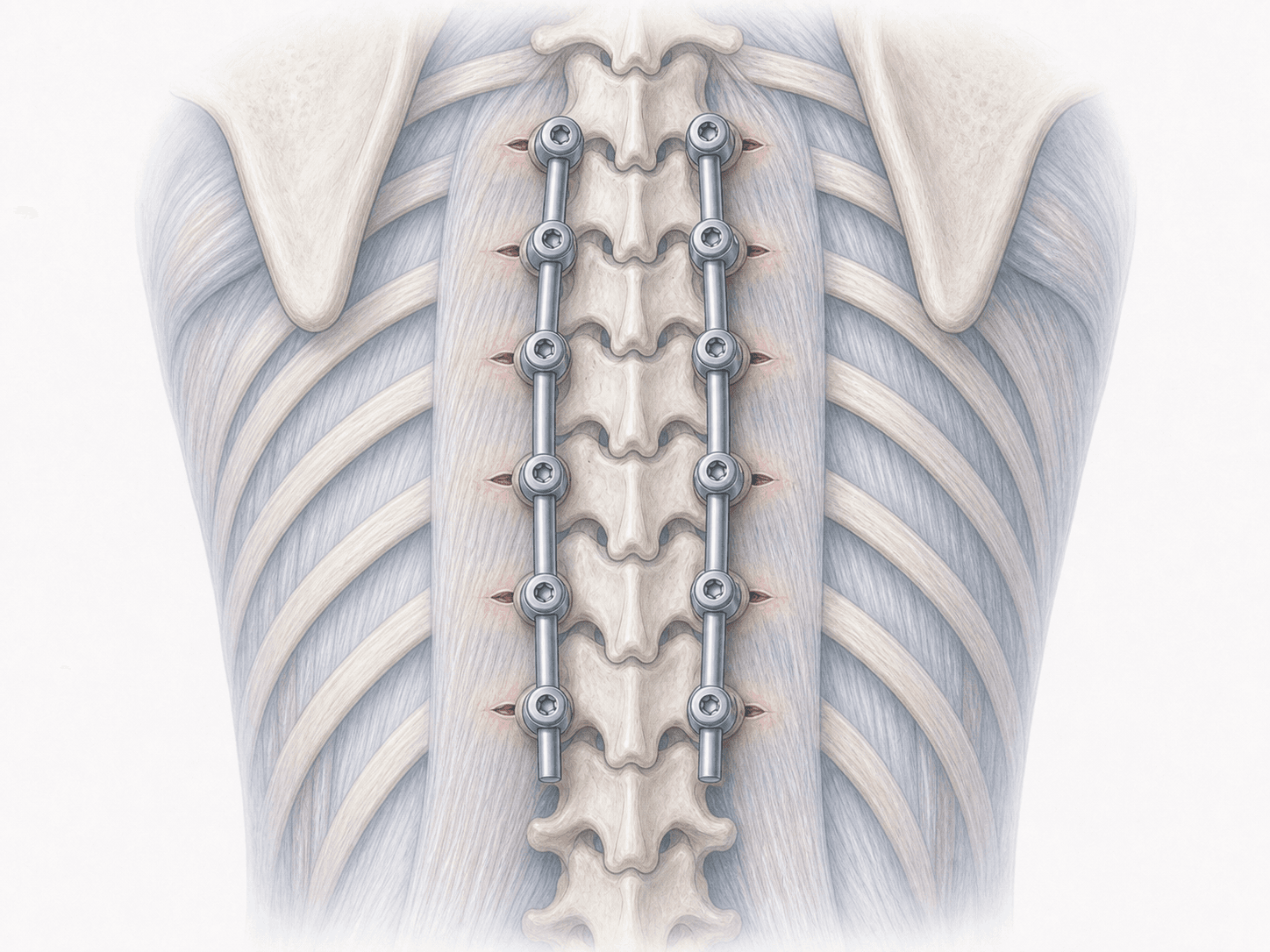
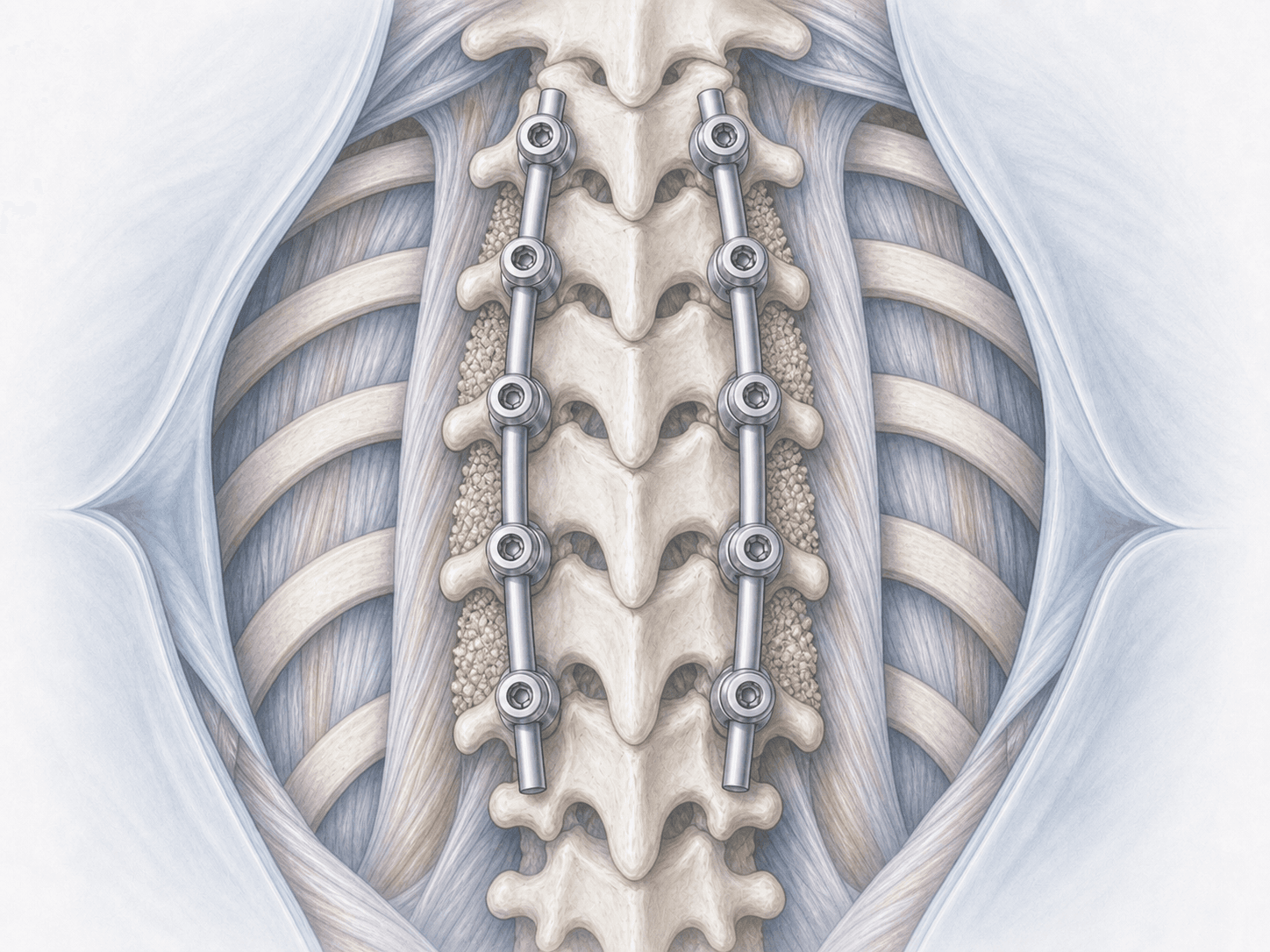
Percutaneous thoracic instrumentation is a minimally invasive surgery in which pedicle screws are placed into the thoracic vertebrae through small skin incisions, without detaching the paraspinal muscles as required in an open approach. The screws are connected by rods that are also introduced percutaneously, providing stability to the affected segment.
Screw placement is performed under fluoroscopy or, preferably, intraoperative navigation (O-arm or similar) to ensure accuracy through the narrow thoracic pedicles.
Compared to a traditional open posterior thoracic fusion, this technique allows stabilisation of fractures, metastases or infections with less blood loss, less postoperative pain and a quicker recovery. To assess whether your case is suitable, you can request an assessment with Dr. Ben Ghezala.
Symptoms and warning signs
Patients who may benefit from percutaneous thoracic instrumentation typically report:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
Includes clinical assessment, review of MRI and fine-cut CT scans to plan screw size and trajectory, and a detailed explanation of the procedure. Fasting instructions, medication adjustments (especially anticoagulants and antiplatelets) and recommendations tailored to the patient's general condition are provided.
2.During the procedure
Under general anaesthesia and in the prone position, several small skin incisions (about 1.5–2 cm) are made on each side of the midline, over the levels to be fixed. Through each incision, and under fluoroscopic guidance or intraoperative navigation, a pedicle screw is placed in the corresponding vertebra, crossing the muscle without detaching it. Once all screws are in place, the connecting rods are also passed percutaneously and the locking caps are tightened to provide final stability.
3.Immediate postoperative period
After surgery, patients spend a short time in recovery before returning to their room. Postoperative pain is usually noticeably less than after open surgery and is managed with standard analgesia. Early mobilisation, often on the same day or the day after surgery, is one of the main benefits of the technique. Hospital stay is typically 2–4 days depending on clinical progress.
Recovery after percutaneous thoracic instrumentation
Recovery after this technique is usually faster than after an equivalent open surgery, because the paraspinal muscles are largely preserved and the incisions are small, which reduces postoperative pain and visible scarring.
Most patients walk within the first 24–48 hours and resume basic daily activities within 1–2 weeks. Returning to a sedentary job typically occurs between 4 and 6 weeks, while physical jobs require additional time and are assessed individually.
Rehabilitation is introduced progressively, avoiding heavy strain during the first weeks. Clinical and radiological follow-up confirms correct positioning of the instrumentation. Fever, severe pain or new neurological symptoms warrant prompt medical review.
Risks and possible complications
Any surgery carries general risks such as infection, bleeding, anaesthesia-related issues or thrombosis, although blood loss and infection rates are typically lower than with open surgery.
Specific risks of percutaneous thoracic instrumentation include screw malposition (more relevant in upper thoracic pedicles, especially without navigation), injury to a nerve root or adjacent vessels, cerebrospinal fluid leak, pneumothorax at high thoracic levels, loosening or breakage of the instrumentation and the rare need to convert to open surgery. These risks are assessed individually and intraoperative navigation significantly reduces them.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala