Failed lumbar fusion revision (lumbar pseudarthrosis)
Revision of a failed lumbar fusion is indicated when a previous lumbar arthrodesis has not achieved bony consolidation (lumbar pseudarthrosis) and mechanical back pain persists, screws or cages loosen or radicular symptoms reappear. We understand how disheartening it is to remain in pain after a surgery that was meant to be definitive and how unsettling it feels to consider a second operation. Our role is to offer a careful second-opinion assessment, reviewing your previous reports, current imaging and clinical course to understand what has failed and what can be done. This guide summarises when revision should be considered, the available technical options and what to expect from the lumbar salvage process.
What is the revision of a failed lumbar fusion?
Revision of a failed lumbar fusion is a salvage operation aimed at treating a previous lumbar arthrodesis that has not consolidated. When bone fails to bridge the operated segment the condition is called lumbar pseudarthrosis. The treated level remains abnormally mobile, mechanical back pain returns or never fully resolves and, in some cases, the pedicle screws or interbody cages become loose or migrate.
This is a familiar scenario for our team. Dr. Ben Ghezala has authored dedicated chapters on lumbar pseudarthrosis and on the use of bone morphogenetic proteins (BMP) in reference German textbooks such as Spinale Neurochirurgie (Schattauer, 2009) and Wirbelsäule Interdisziplinär (Schattauer/Thieme, 2017), which guides planning when a first surgery has not met its goals.
The strategy depends on each case. In many patients the answer is to reinforce the fusion through a posterior approach, removing or replacing loose pedicle screws, extending the arthrodesis with bone graft and, in selected cases, performing a new transforaminal lumbar interbody fusion (TLIF). In others an anterior approach is added to place a large interbody cage and achieve circumferential structural support. When poor bone quality, multiple levels or sagittal imbalance coexist, a combined anterior plus posterior strategy is considered, with biological support through autologous graft or, in selected scenarios, BMP.
To review your case, you can request a second opinion with Dr. Ben Ghezala. If you want to better understand the interbody technique often used in these salvage procedures, you can read more about TLIF — transforaminal lumbar interbody fusion.
Symptoms and signs of a failed lumbar fusion
After a lumbar fusion, certain signs should raise suspicion of pseudarthrosis or hardware failure:
When is revision surgery indicated?
How is the procedure performed?
1.Preoperative preparation
Preparation includes a complete review of the previous surgery: operative report, implant type, number of fused levels and postoperative course. Fine-cut lumbar CT to rule out pseudarthrosis, MRI to assess neural tissue and adjacent levels, and flexion-extension X-rays are usually requested. Bone quality (with bone densitometry if appropriate), hardware status and the presence of kyphosis or sagittal imbalance are assessed, and alternative causes of pain such as low-grade chronic infection are ruled out. Medication is adjusted, postoperative analgesia is planned, smoking cessation is addressed when relevant (a critical factor for non-union) and the chosen strategy and alternatives are explained in detail.
2.During the procedure
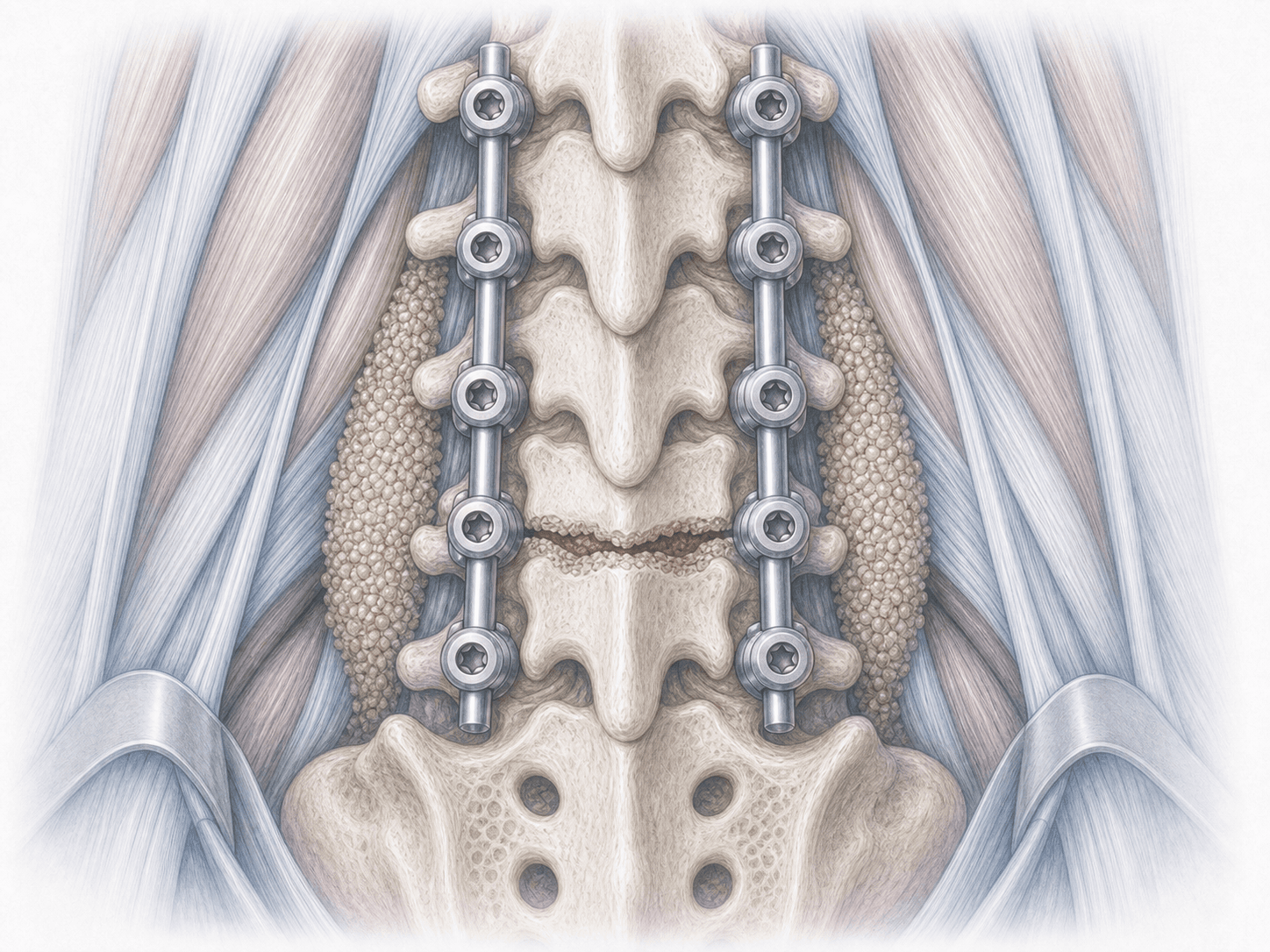
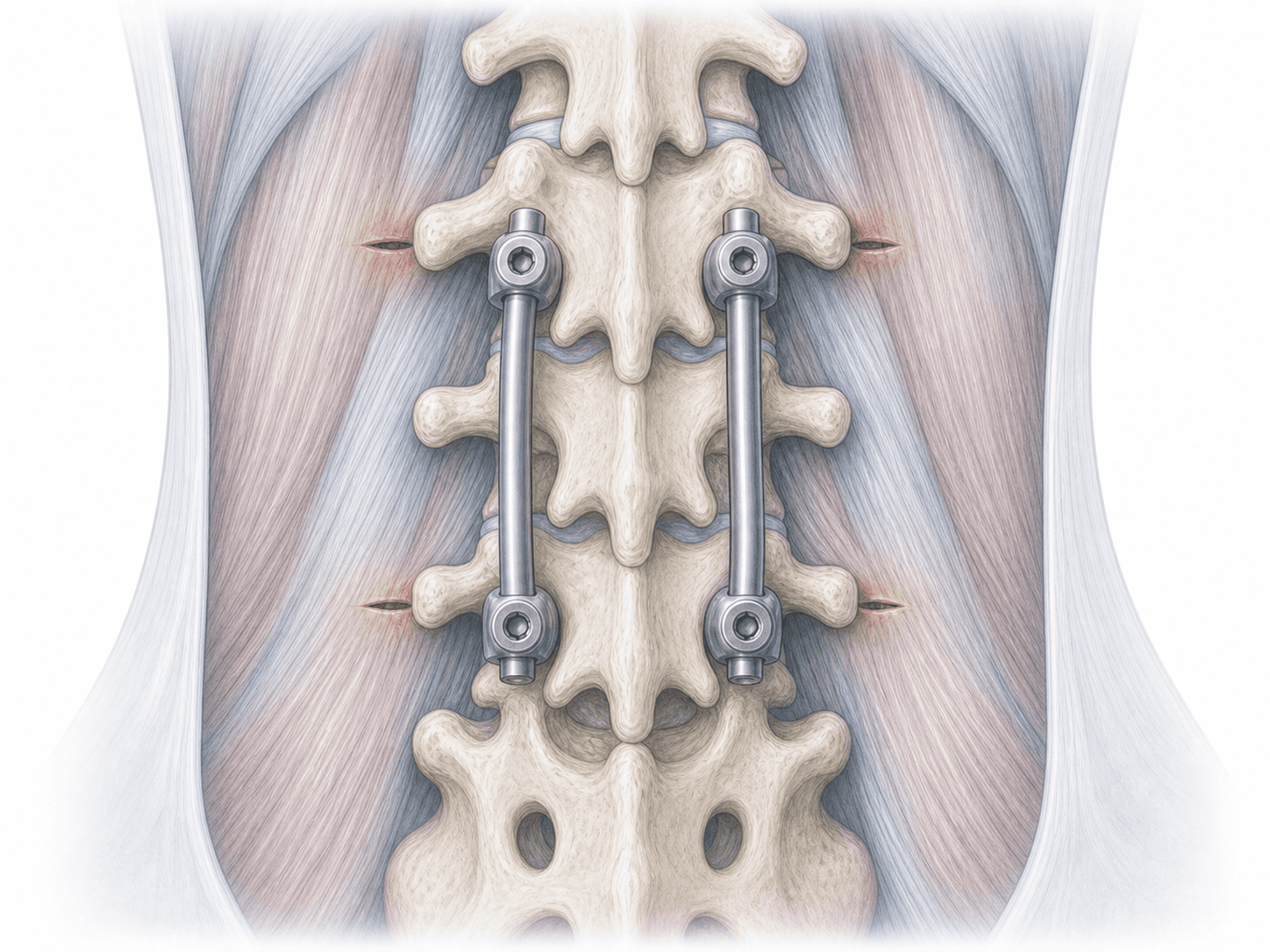
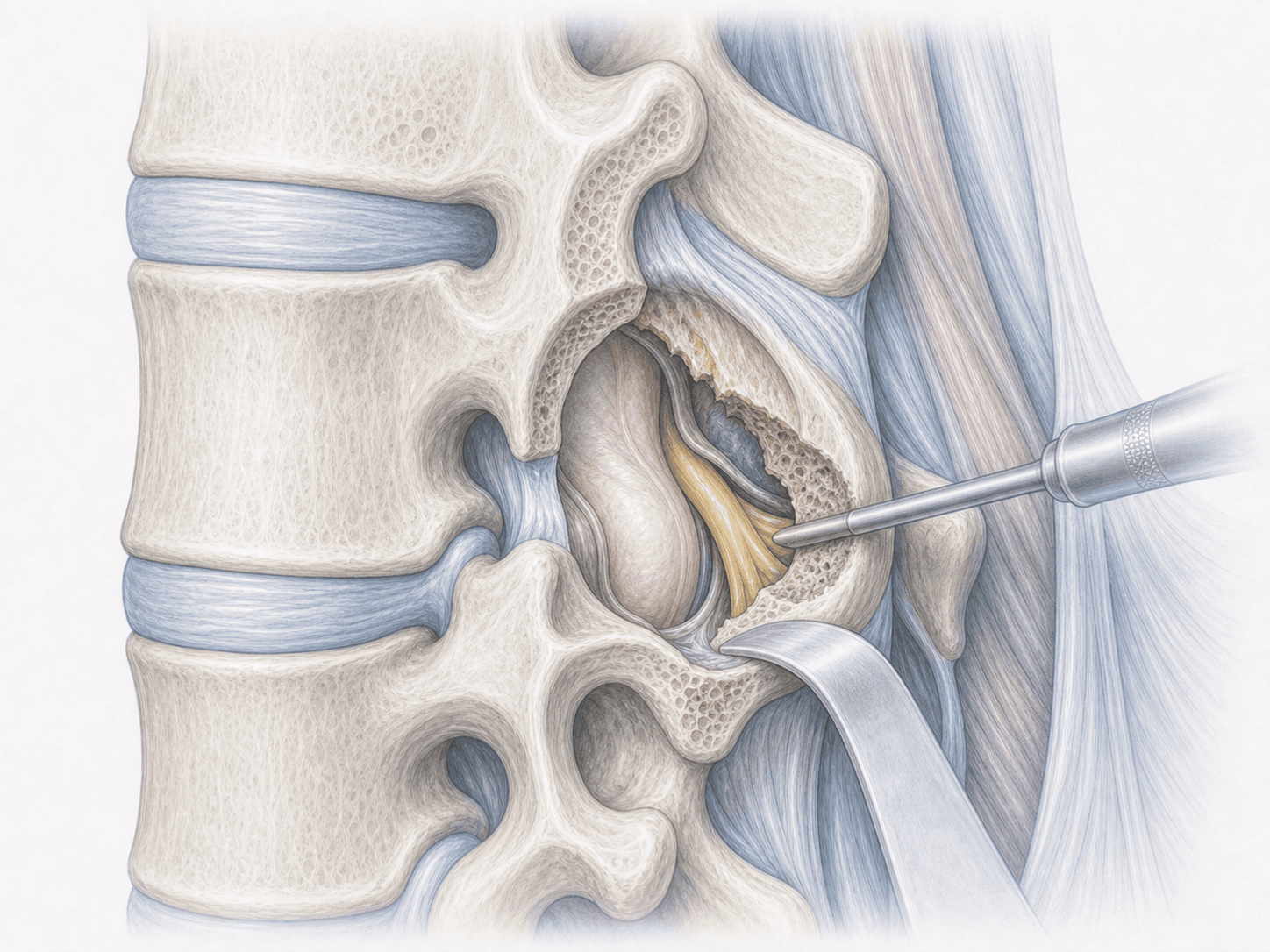
The procedure is performed under general anaesthesia, in the prone position and, in complex approaches, with neurophysiological monitoring. If a posterior-only revision is chosen, the previous scar is used to access the spine, fibrous tissue is removed, pedicle screws are exposed and any loose screws are replaced with larger-diameter or cement-augmented screws; the arthrodesis is extended with autologous graft (iliac crest or local bone) and, in selected cases, a new transforaminal interbody fusion (TLIF) is performed.
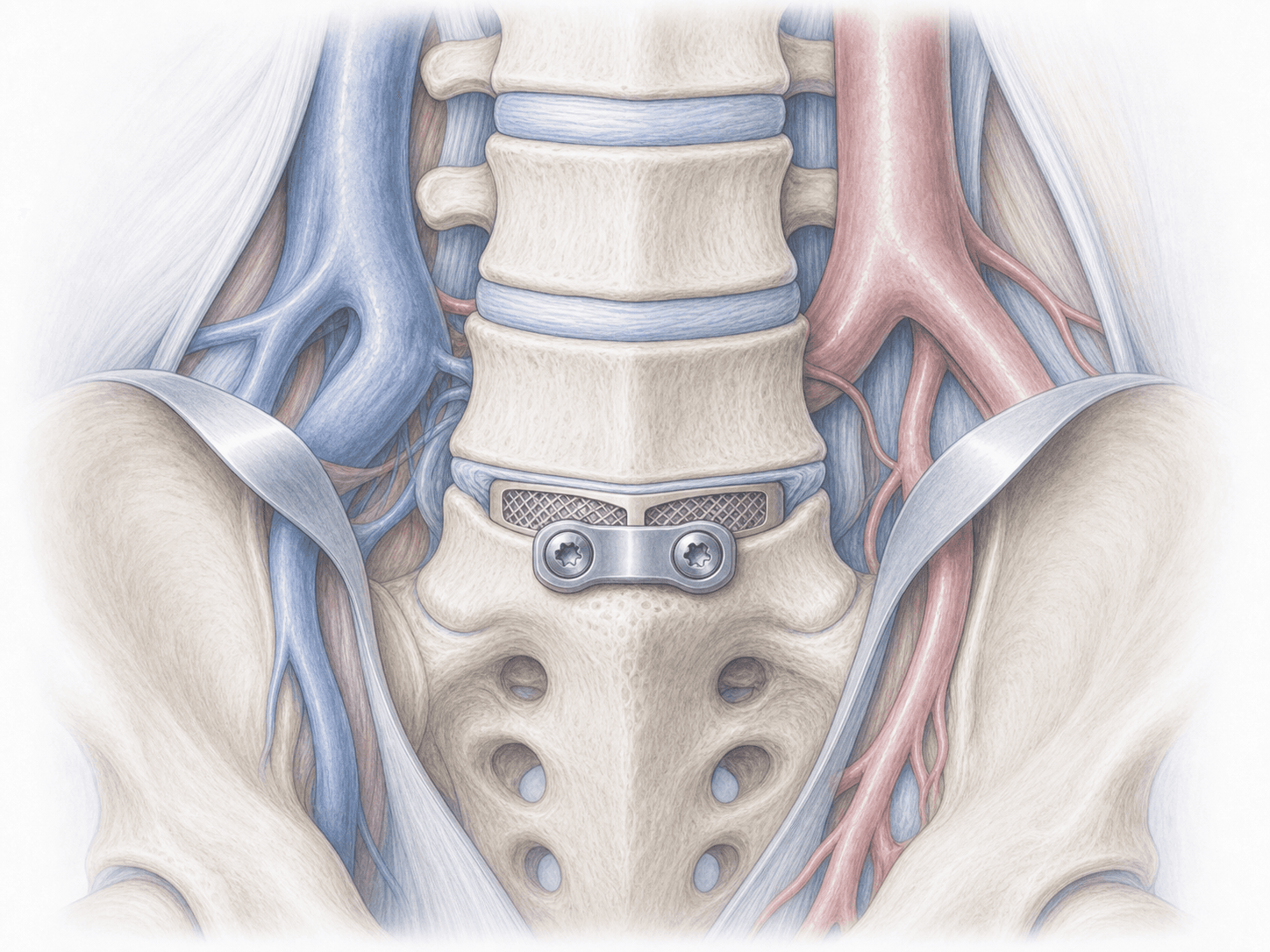
In a circumferential strategy (anterior plus posterior), an initial anterior stage allows removal of the previous interbody implant when needed and placement of a larger cage with good bone contact, restoring disc height and lordosis. A subsequent posterior stage, in the same session or staged, reinforces the fusion with pedicle instrumentation and adds more graft. In selected scenarios of recurrent pseudarthrosis or poor bone quality, bone morphogenetic proteins (BMP) may be considered as a biological adjunct to the graft.
3.Immediate postoperative period
After surgery the patient spends a short time in the recovery area before returning to the ward. Pain is controlled, a postoperative X-ray or CT is obtained to verify the position of the new instrumentation and progressive mobilisation begins, usually supported by a lumbar brace during the first weeks. Hospital stay is typically 3–6 days, slightly longer than in primary surgery, depending on the complexity of the salvage, whether a circumferential approach has been used and the clinical course.
Recovery after lumbar revision surgery
Recovery after a lumbar revision is slower than after primary surgery. Daily activities are gradually resumed within a few days, initially avoiding prolonged sitting or lifting. Office work usually restarts between 6 and 8 weeks; physical jobs require more time and an individual assessment.
Bony fusion takes several months to consolidate and is often slower in a revision than in a first surgery. Heavy strain, impact sports and axial loading are avoided during the first three to six months. Guided rehabilitation, good postural hygiene, smoking cessation, diabetes control and clinical-radiological follow-up are key to achieving a stable fusion. Fever, severe pain, wound discharge or new neurological symptoms warrant prompt medical review.
Risks and possible complications
Any surgery carries general risks such as infection, bleeding, thrombosis or anaesthesia-related complications. Lumbar revision surgery adds extra risk due to scar tissue, the presence of previous implants, loss of anatomical landmarks and the longer duration of the procedure.
Specific risks include nerve root injury, dural tear with cerebrospinal fluid leak (more frequent in revisions than in primary surgery), vascular injury in anterior approaches, postoperative haematoma, deep infection, persistent pseudarthrosis requiring further salvage, loosening or fracture of the new instrumentation, residual chronic pain and accelerated adjacent-segment degeneration. Each patient receives an individualised assessment to minimise these risks and realistic expectations about the outcome are discussed honestly.
Frequently asked questions
Other related treatments

Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala