Post-traumatic cervical instability stabilization
After a car crash, a fall from height or a severe whiplash, the ligaments that hold the cervical spine together can tear even when the bones look intact on the first X-ray. When that happens, the neck loses its stability and the spinal cord becomes exposed to damage that may appear hours or days later. Surgical stabilization restores mechanical support to the injured segment using screws, rods or cages, and protects the spinal cord before a neurological deficit develops. This guide explains when urgent surgery is needed, how the approach is chosen and what to expect during recovery, with the same information we share in consultation with patients and their families.

What is post-traumatic cervical instability stabilization?
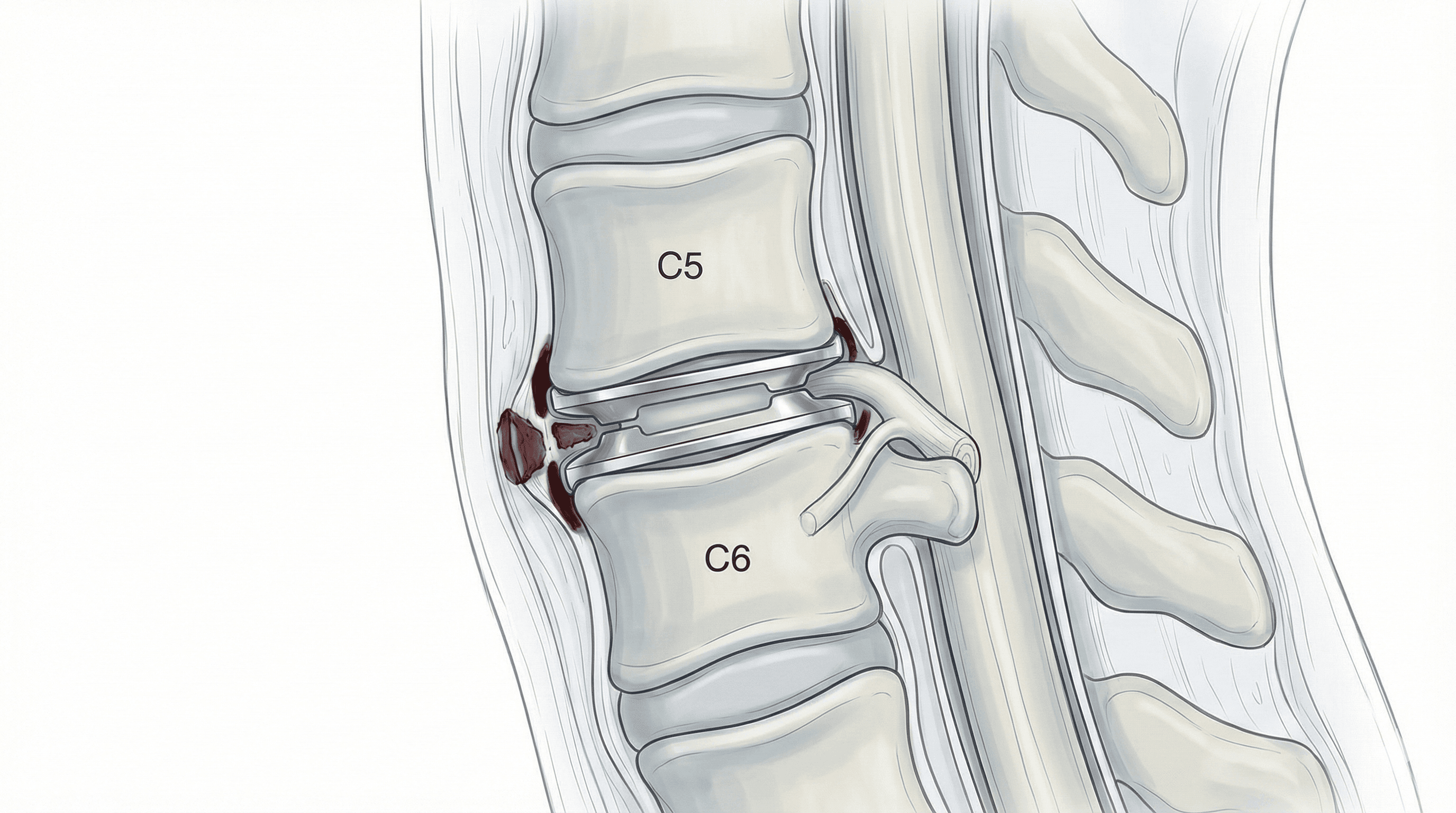
This surgery restores mechanical stability to the neck when a severe injury has torn the ligaments, disc or joints that keep the vertebrae aligned. It is performed after road traffic crashes, falls from height, sports impacts or severe whiplash with confirmed structural damage.
The goal is twofold: to protect the spinal cord from further displacement and to allow the injured segment to heal in a stable position. Depending on the injury pattern, the type of fracture and the affected level, we choose an anterior approach with cage and plate, a posterior approach with lateral mass or pedicle screws, or a combined approach. When there is also a loss of vertebral body height, it can be combined with a posterior cervical fusion or a corpectomy.
If a family member has had a recent accident with suspected cervical injury, you can request an urgent assessment with Dr. Ben Ghezala.
Symptoms and warning signs after trauma
Post-traumatic cervical instability can appear immediately or develop over days. In the first hours or days after the accident, watch for:
When is surgical stabilization indicated?
How is the procedure performed?
1.Preoperative preparation
Before surgery we review the MRI, CT and dynamic X-rays to classify the injury and decide the approach. Full blood work and anaesthesia assessment are completed and, if needed, a rigid collar or halo vest is used to immobilise the neck until theatre. In urgent cases, surgery can be scheduled within hours if there is risk to the spinal cord.
2.During the procedure
Surgery is performed under general anaesthesia and, in most cases, with intraoperative neurophysiological monitoring to watch the spinal cord in real time. Depending on the injury pattern, we use an anterior approach to remove the torn disc and place a cage and plate, a posterior approach with lateral mass screws (C3 to C6) or pedicle screws (C7) linked by rods, or both when there is combined anterior and posterior disruption. Reduction of the dislocation is completed before the segment is fixed.
3.Immediate postoperative period
After surgery the patient spends a few hours in recovery and, depending on severity, may need intensive care during the first day. A postoperative CT scan is performed to confirm implant position. Mobilisation with a soft collar starts early and the hospital stay is usually 3 to 5 days, longer if there was a preoperative neurological deficit.
Recovery after post-traumatic cervical stabilization
Recovery depends on the preoperative neurological status and the number of levels fixed. For the first 6 weeks a collar is worn and lifting, driving and sudden movements are avoided. Bony fusion takes 3 to 6 months, during which the segment is protected by the instrumentation.
Physiotherapy is introduced step by step, first focused on posture and shoulder mobility and later on neck strength. Return to office work usually happens between 6 and 12 weeks; physical jobs and contact sports require complete fusion and specific clearance. Fever, wound discharge, severe pain or new neurological symptoms warrant immediate review.
Risks and possible complications
All surgery carries general risks such as infection, bleeding, thrombosis or anaesthesia-related issues. Urgent cervical surgery adds its own risk profile because of the proximity of the spinal cord and vascular structures.
Specific risks include injury to the spinal cord or a nerve root, vertebral artery injury, oesophageal or tracheal injury in anterior approaches, transient swallowing difficulty, screw malposition or loosening, non-union (pseudarthrosis) and accelerated degeneration of adjacent levels. In patients with a preoperative neurological deficit, surgery stabilises the spine but does not always reverse damage already established.
Frequently asked questions
Other related treatments



Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala