Multilevel cervical stenosis surgery
Multilevel cervical stenosis surgery (narrow cervical canal at multiple levels) is considered for people with neck pain and stiffness, tingling in arms and hands and often walking difficulty or hand clumsiness. Imaging shows a narrow cervical canal at several levels, leaving little space for the cord and risking progressive damage. When symptoms worsen and conservative care is no longer enough, surgery aims to decompress the cord and nerve roots to slow progression. Indication is personalised based on symptoms, neurological exam and imaging.

What is multilevel cervical stenosis surgery?
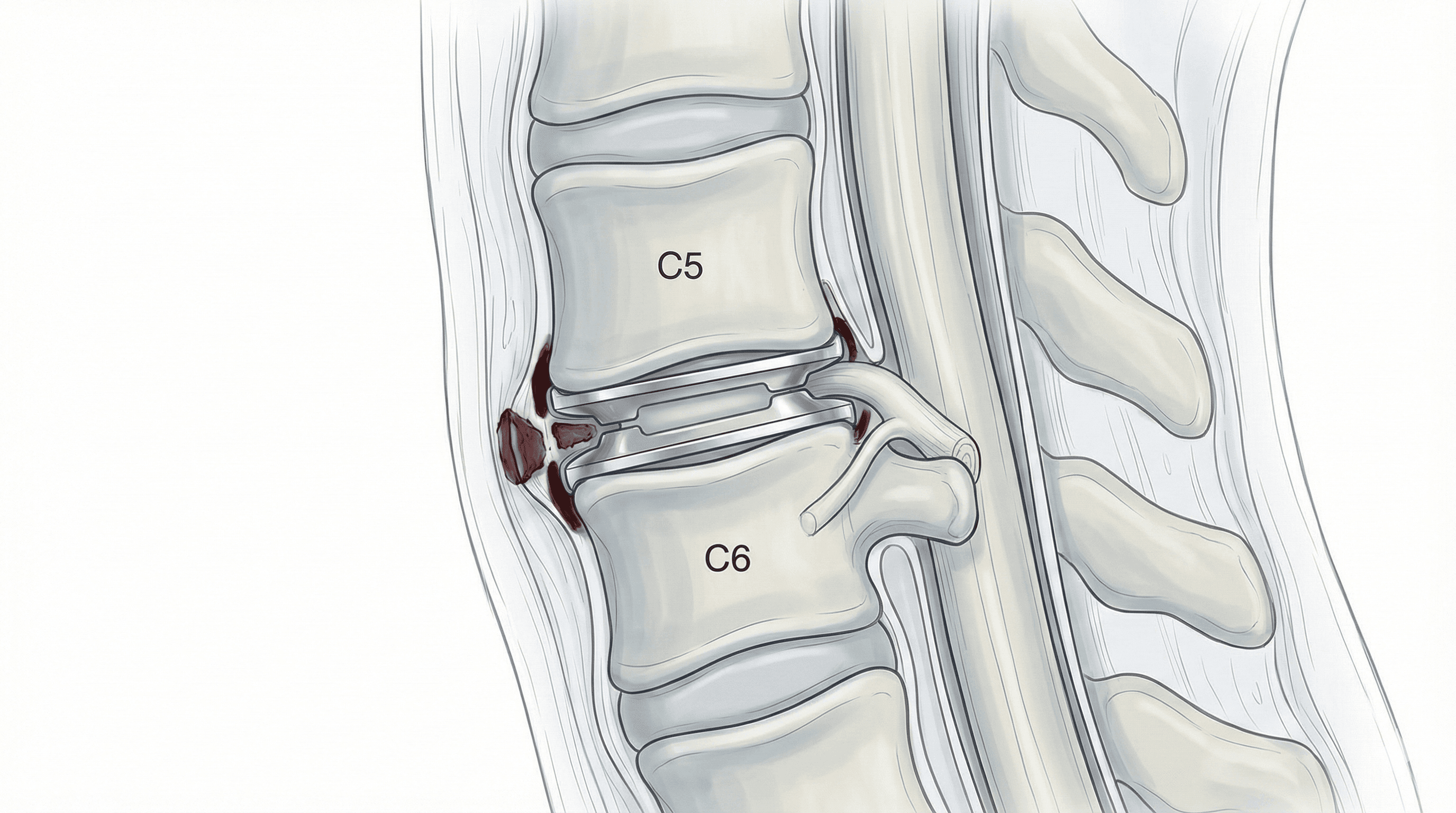
Multilevel cervical stenosis surgery includes techniques to enlarge the cervical canal and provide more space for the cord and nerve roots when narrowing affects several levels. Stenosis is often caused by advanced arthritis, thickened ligaments, multiple disc herniations or ossifications that markedly reduce canal diameter. Depending on the pattern, decompression may be anterior (acting on discs and vertebral bodies), posterior (laminectomy, laminoplasty) or combined, treating discs, vertebral bodies, laminae and ligaments compressing the cord and roots. Unlike more limited procedures focused on one level or root, it tackles a broader problem common in multilevel cervical myelopathy, where protecting neurological function is the priority.
Symptoms and warning signs
Multilevel cervical stenosis may progress slowly. Watch for these symptoms:
When is this procedure indicated?
How is the procedure performed?
1.Preoperative preparation
A thorough clinical and neurological assessment is performed with detailed MRI/CT review to define levels, stenosis pattern and strategy (anterior, posterior or combined). The neurosurgeon explains goals, alternatives, possible outcomes and risks, answering patient and family questions. Fasting instructions are given, medication is reviewed (especially anticoagulants and antiplatelets) and comorbidities are assessed with anaesthesia before consent.
2.During the procedure
Performed under general anaesthesia. Anterior approaches reach the spine from the front of the neck, removing discs and sometimes vertebral bodies (corpectomies) compressing the cord, and placing cages, grafts and plates to maintain space and stabilise. Posterior approaches use laminectomy or laminoplasty to widen the canal from behind and may add fixation with screws and rods. In some cases both approaches are combined to achieve complete decompression and proper alignment.
3.Immediate postoperative period
After surgery, the patient spends time in recovery where breathing, blood pressure, neurological status and pain are monitored, then returns to the ward. Mobilisation usually starts progressively the next day with physiotherapy to stand and walk safely. Strength, sensation and gait are monitored. Typical hospital stay is 3–5 days, adjusted to complexity and individual course.
Recovery and daily life
Recovery is gradual. In the first days, neck pain, stiffness and fatigue are common; basic mobilisation starts early under supervision. Neurological improvement may be progressive and sometimes partial: the main goal is to stop or slow decline and recover function when possible.
Return to office work is often considered between 6 and 8 weeks; physical jobs or those with fall risk may require 3–4 months or more. Physiotherapy, gait retraining, cervical and back strengthening, and ergonomics at home and work are key. If fever, severe pain, new weakness or sudden gait worsening occurs, prompt review is needed.
Risks and possible complications
As with any spine surgery involving the cord, there are risks. General risks include anaesthesia-related problems, infection, bleeding, haematoma and venous thrombosis.
Specific risks include spinal cord or nerve root injury that could worsen strength or sensation, persistence or lack of myelopathy improvement, instability if not stabilised properly, pseudoarthrosis when fusion is performed, residual or chronic neck pain and long-term cervical alignment changes. In complex cases, the extent of surgery may increase recovery time. These risks are weighed against the risk of not operating, which in severe stenosis can mean progressive neurological decline.
Frequently asked questions
Other related treatments



Do these symptoms sound familiar?
If you recognise yourself in some of these symptoms and your pain is starting to limit your daily life, we can review your case in a personalised consultation. Dr. Ben Ghezala will assess your clinical history and imaging studies to help you decide the best treatment option for you.
Request a consultation with Dr. Ben Ghezala